NOTE: All procedures described in this paper are performed according to guidelines established by the Stanford Administrative Panel on Laboratory Animal Care (APLAC).
1. Timed Pregnancies – Superovulation Technique (Figure 1)
NOTE: Precisely timing the gestational age of mouse embryos for fetal surgery at E16.5 and E18.5 is of critical importance. In this section we detail our protocol for timing mouse pregnancies using pregnant mares serum (PMS) and human chorionic gonadotropin (HCG) injections to induce superovulation.
- Inject female mice (<5 per cage) intraperitoneally (IP) with 3.0-5.0 international units (IU) of PMS in a volume of 100 μl PBS between 1:00 and 3:00 PM for day 1.
- Between 12:00 and 2:00 PM of day 3 (forty-five to 47 hr after PMS injection), inject female mice IP with 3.0-5.0 IU of HCG in a volume of 100 μl PBS.
NOTE: The HCG injection induces ovulation approximately 12 hr post-injection. - Immediately following HCG injections, mate females with males aged 8-16 weeks.
NOTE: We typically place two females into a cage of individual males. - Separate females from males on the morning of day 4 (6:00 – 10:00 AM) and record as fetal age E0.5.
NOTE: Vaginal plugs can be checked at this time; however, the observation of a vaginal plug does not guarantee pregnancy and females can become pregnant when no plug is observed. Given that pregnancy is typically observable by visual inspection and/or palpation at gestational ages E16.5 and E18.5, checking for vaginal plugs on the morning of day 4 is not strictly necessary. In our experience, and depending on the strain, approximately 30-50% of super-ovulated females become pregnant using the technique described here.

Figure 1. Schematic for Superovulation Technique. Schematic showing procedure for superovulation timed pregnancies in mice. Please click here to view a larger version of this figure.
2. Murine Fetal Surgery (Dorsal Wounding) on E16.5 and E18.5 Embryos (Figure 2)
- Before the procedure, clean all surfaces of the operating room and equipment with 70% isopropyl alcohol. In addition, sterilize all surgical supplies and instruments that will be used in the procedure by autoclaving them. Some institutions may allow subsequent use of hot bead sterilization. Per operation, use sterile packs that include gauze and surgical instruments.
- Induce anesthesia in pregnant mothers (fetal age E16.5 or E18.5) under 2.5% isoflurane/oxygen mixture at 2 L per min followed by maintenance anesthesia at 1 L per min.
- To confirm proper anesthetization, ensure the deep pedal reflexes of the mouse are suppressed and place the mouse in the prone position.
- Apply a vet ophthalmic ointment such as Puralube to prevent eye irritation or dryness during the procedure.
- Prepare abdomen by administering a light application of depilatory cream for no longer than 30 sec (Figure 2A).
- Prepare abdomen for aseptic surgery with povidone-iodine and alcohol (Figure 2B and 2C).
- Perform midline laparotomy under microscope using microsurgical scissors (Figure 2D and 2E).
- Gently expose uterus and fetus selected for surgery (Figure 2F).
- Irrigate surgical field with warm (38 °C) phosphate-buffered saline (PBS) using a blunt-tip needle
NOTE: One can be made by carefully bending the tip of a large-bore needle. (Figure 2G and 2H). - Position the fetus in a manner that allows full access to dorsum.
- Pass a purse string stitch using 7-0 nylon suture through the uterus overlying the site of intended dorsal wounding (Figure 2I). Position purse string over a region of dorsum to the left or right of spinal cord, and in a region of uterine wall devoid of large blood vessels.
- Make a 3 mm incision through uterine wall and amniotic sac in the center of the purse string (Figure 2J).
- Irrigate incision site with warm (38 °C) PBS.
- Using microsurgical scissors, cut a single full-thickness excisional wound, approximately 1 mm in length, in the dorsum of the fetus.
- Gently blot incision site dry with cotton-tip applicator.
- Inject 3 μl volume India ink subcutaneously into the wound site to mark location of wound (Figure 2K).
- Irrigate with warm (38 °C) PBS to ensure ink has been retained within wound site.
- Have surgical assistant inject warm (38 °C) PBS through blunt-tip 10 G syringe into the amniotic sac as the purse string is closed ( Figure 2L). Retract syringe as purse string closure nears completion (Figure 2M).
- Gently return uterus into the abdominal cavity (Figure 2N).
- Evert skin and peritoneum.
- Have surgical assistant irrigate abdominal cavity with warm (38 °C) PBS.
- Close abdomen quickly by stapling skin and peritoneum closed (Figure 2O). The standard closure is performed in two layers; peritoneum and abdominal muscle in one layer, subcutaneous tissue and skin in the second layer. For immediate sacrifice and harvesting of the fetus, our demonstration shows closure in one layer.
- Place the animal under observation in a warm incubator set at 37 °C for 30 min or until the animal regains sufficient consciousness to maintain sternal recumbency.
- Do not return the animal to the company of other animals until it has fully recovered from the procedure.
- Upon awaking from anesthesia and during the subsequent 48 hr, administer subcutaneous injection of buprenorphine (0.05 mg/kg) every 12 hr for analgesia as needed based on pain assessment. Administer carprofen (5 mg/kg) via subcutaneous injection for additional post-operative pain relief as needed.
- Return animals to the cage and provide them with food and water ad libitum.
- Monitor closely for manifestations of pain.
- 48 hr post-surgery, sacrifice pregnant mother with an overdose of isoflurane and harvest wounded fetus. In order to do this, adjust isoflurane concentration to 5% or higher and maintain exposure for 1 min after cessation of breathing. Confirm euthanasia with cervical dislocation. Harvest an unwounded embryo for age-matched control. Late embryos should have a separate method of euthanasia consistent with IACUC recommendations, such as decapitation, cervical dislocation, or chemical injection.
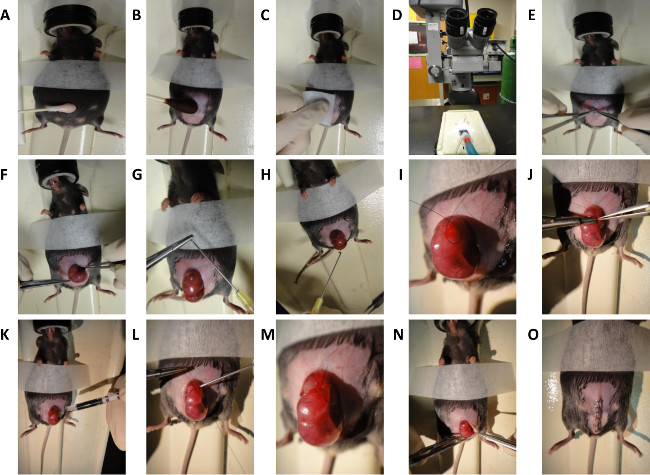
Figure 2. Schematic for Murine Fetal Surgery. General steps for dorsal wounding in E16.5 and E18.5 mouse embryos. (A) Depilation of mouse abdomen. (B and C) Preparation of mouse abdomen. (D) Microscope used for surgical procedure. (E) Midline laparotomy. (F) Exposure of uterus. (G) Creation of blunt-tip needle. (H) Irrigation of uterus with warm saline. (I) Creation of purse string suture. (J) Incision through uterine wall and 1 mm full thickness excisional wound generation. (K) Subcutaneous injection of India ink. (L and M) Closure of purse string suture. (N and O) Closure of abdomen. Please click here to view a larger version of this figure.
For histologic analysis, cutaneous wounds in the dorsal skin of E16.5 and E18.5 mouse embryos should be harvested 48 hr post-wounding, fixed in 4% PFA, and paraffin-embedded. In fluorescent transgenic models, cryopreservation with OCT may be appropriate. There are several stains that may be used to visualize cellular and connective tissue architecture. Hematoxylin and eosin is a two-color stain that stains nuclei blue and eosinophilic structures (i.e., cytoplasm and extracellular collagen) various shades of red, pink, and orange. Mallory’s trichrome is a three-color stain consisting of aniline blue, acid fuschin and orange G, best suited for distinguishing cells from surrounding connective tissue.
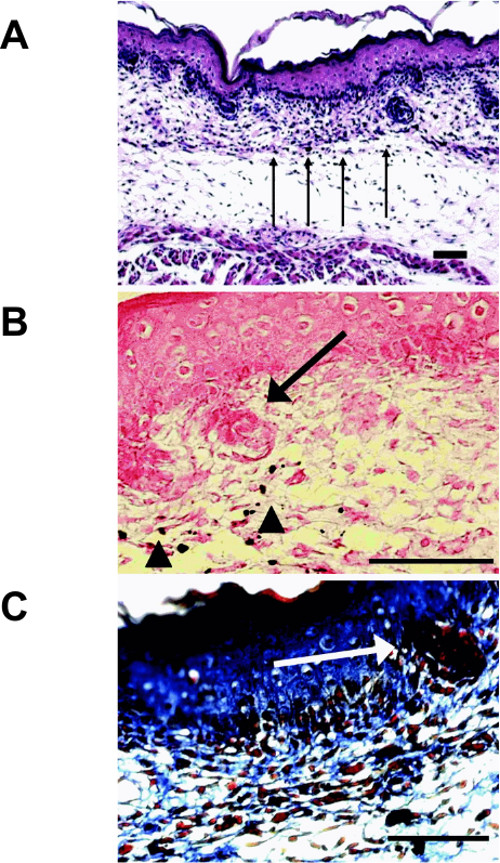
Figure 3. Histology of Scarless E16.5 Fetal Wounds. (A) Hematoxylin and eosin stain reveals complete reepithelialization and a mild increase in the number of inflammatory cells present (arrows) (100x; bar = 100 μm). (B) Eosin stain shows India ink (arrowheads) around regenerating hair follicles (arrow) (400x; bar = 25 μm). (C) Mallory’s trichrome stain reveals a fine reticular dermal collagen pattern with the presence of a hair follicle (400x; bar = 25 μm). Reprinted with permission from Colwell et al.10 Please click here to view a larger version of this figure.
If dorsal excisional wounds are of the appropriate size (1 mm) and depth (full-thickness), hematoxylin and eosin staining will reveal that E16.5 skin heals with minimal scarring, complete reepithelialization, and only a small increase in the number of inflammatory cells (Figure 3A). Moreover, these wounds should heal with approximately normal skin architecture and contain regenerating hair follicles within the site of injury (arrows; Figure 3B). Proper application of india ink to the freshly created wound should result in ink deposition at the site of injury (arrow heads; Figure 3B). Finally, trichrome staining should reveal a fine reticular dermal collagen pattern characteristic of unscarred dermis (Figure 3C).
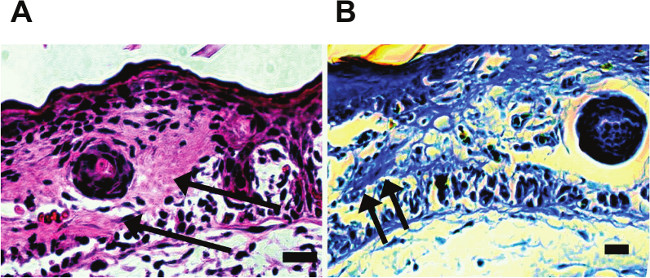
Figure 4. Histology of Scarring E18.5 Fetal Wounds. (A) Hematoxylin and eosin stain reveals an increase in eosin staining in the dermis at the site of injury (arrows) (200x; bar = 50 μm). (B) Mallory’s trichrome stain shows dense dermal collagen (arrows) (400x; bar = 25 μm). Reprinted with permission from Colwell et al.10
In comparison to wounds made at E16.5, hematoxylin and eosin staining of dorsal wounds made at E18.5 and harvested 48 hr post-wounding should reveal a dense scar with loss of normal skin architecture at the site of injury (Figure 4A). Similarly, trichrome staining reveals a dense pattern of disorganized collagen deposition (arrows; Figure 4B). Please click here to view a larger version of this figure.
