With the protocol described above, it is possible to map the SCBF along a longitudinal spinal cord sagittal segment.
In the intact spinal cord, there appears to be SCBF irregularities within the parenchyma (Figure 12). This can be explained by the variable distribution of radiculo-medullary arteries (RMA) from one animal to another. RMA refers to segmental arteries that reach the anterior spinal artery (ASA) and therefore provide blood supply to the spinal cord parenchyma. In contrast, the radicular arteries correspond to segmental arteries, which do not reach the ASA and therefore do not provide spinal cord blood supply. Therefore, in spinal cord segments where the RMA anastomoses with the ASA, there is more blood flow (as shown in our results).
After SCI, real-time CEU imaging shows a deficiency in circulation at the injury epicenter. The epicenter remains dark (no contrast agent signal), as there is no active blood flow. More detailed analysis of the blood flow using several ROIs shows three unique blood flow territories. First, at the level of the epicenter, the blood flow is the lowest with a mean decrease of about -90%. Second, in the territories adjacent to the epicenter (both rostral and caudal), SCBF was also significantly decreased (ranging from -50% to -80%). Third, in the most remote areas corresponding to intact tissue, SCBF is preserved. The second region corresponds to the “ischemic penumbra zone”, which should be the target of potential neuroprotective therapies. Being able to readily visualize and quantify SCBF changes post-SCI is useful for assessing the efficiency of therapies aimed at reducing tissue ischemia, and therefore highlights the importance of this technique (Figure 13).

Figure 1. The custom-made bone cutter for laminectomies. The thin blade is designed to slide beneath the lamina. Please click here to view a larger version of this figure.
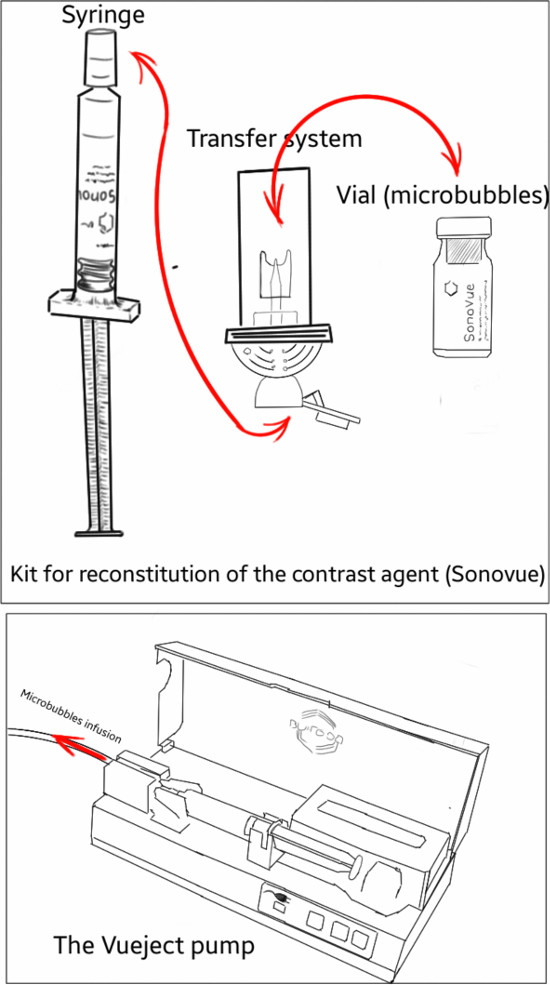
Figure 2. Schematic representation of the kit for microbubbles reconstitution and the Vueject° pump used for microbubbles infusion. The transfer system allows for the delivery of microbubbles and saline between the vial and the syringe. Please click here to view a larger version of this figure.
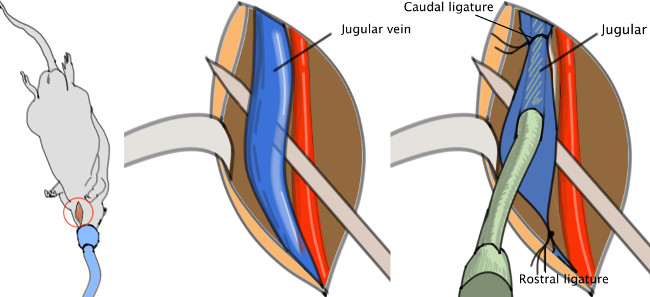
Figure 3. Jugular catheter. The catheter is to be inserted in the jugular vein, then pushed toward the heart and finally fasten with a knot. Please click here to view a larger version of this figure.
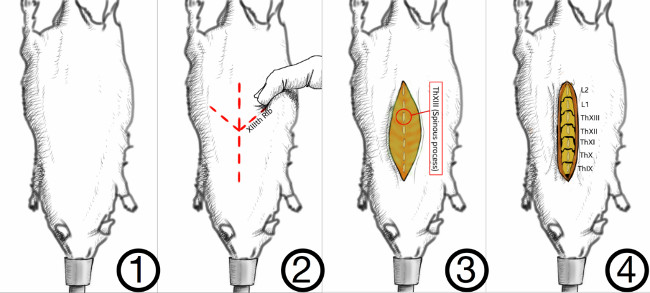
Figure 4. Method for correct identification of the vertebral levels. In the rat, the last rib is attached to the XIIIth vertebra. The latter can be palpated through the skin as a landmark for the last thoracic vertebra, the XIIIth. Muscles are detached on either side of the spinous processes. Please click here to view a larger version of this figure.
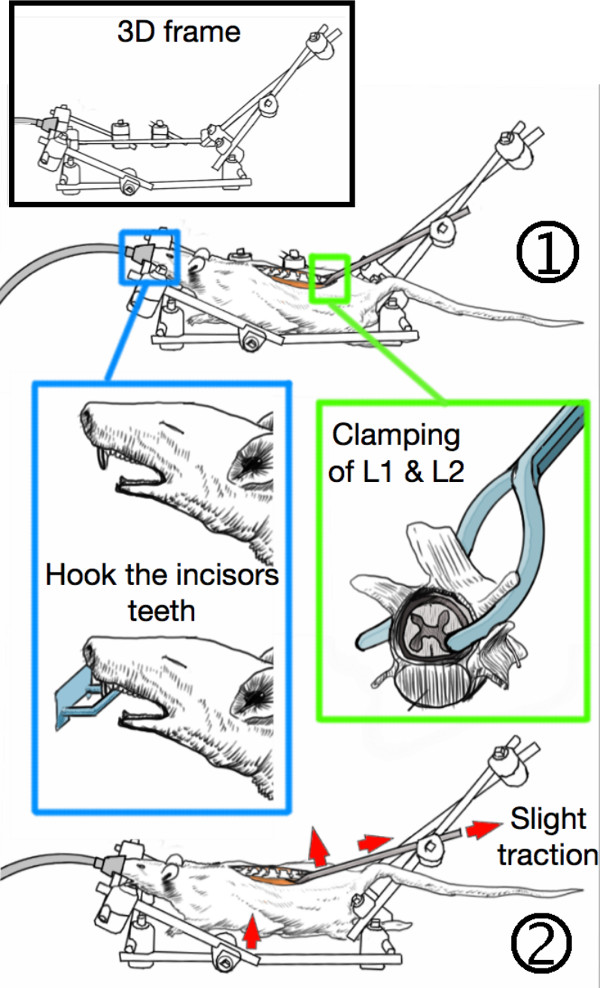
Figure 5. Stabilization of the animal in the 3D-frame. (1) The incisor teeth are hooked on the frame while the first and second lumbar vertebras (L1 & L2) are clamped with custom-made forceps. (2) The lumbar spine is slightly tightened which stabilizes the animal and elevates the thorax from the bench, thereby allowing free respiratory motions without spine movements. Please click here to view a larger version of this figure.
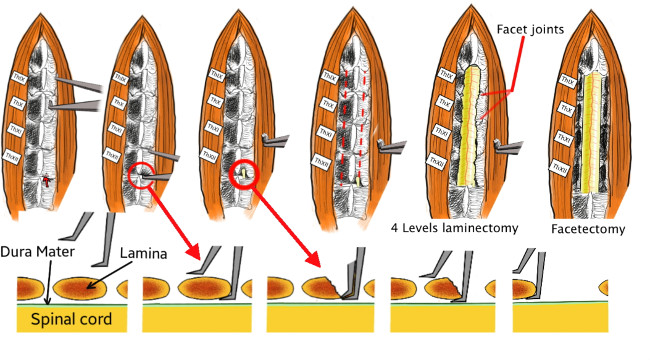
Figure 6. Technical details of the laminectomy. First, the thin blade of the custom-made bone cutter is passed beneath the lamina without damaging the spinal cord. Then the bone cutter is closed, which cuts and removes a part of the lamina. The procedure is repeated on both sides and from ThXII to TxIX in order to achieve a four-level laminectomy. Finally, the facet joints are also removed. Please click here to view a larger version of this figure.
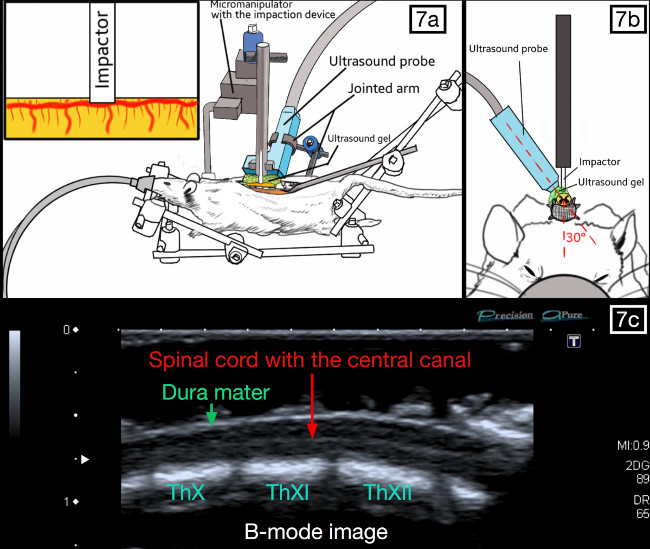
Figure 7. Positioning of the ultrasound probe and the impaction device. The probe is parallel to the spinal cord and slightly oblique (20-30°), so that the weight-drop impactor can be placed against the posterior aspect of the dura. The spinal cord should be visible with the central canal present throughout the middle segment on the ultrasound imaging “B-Mode”. Please click here to view a larger version of this figure.
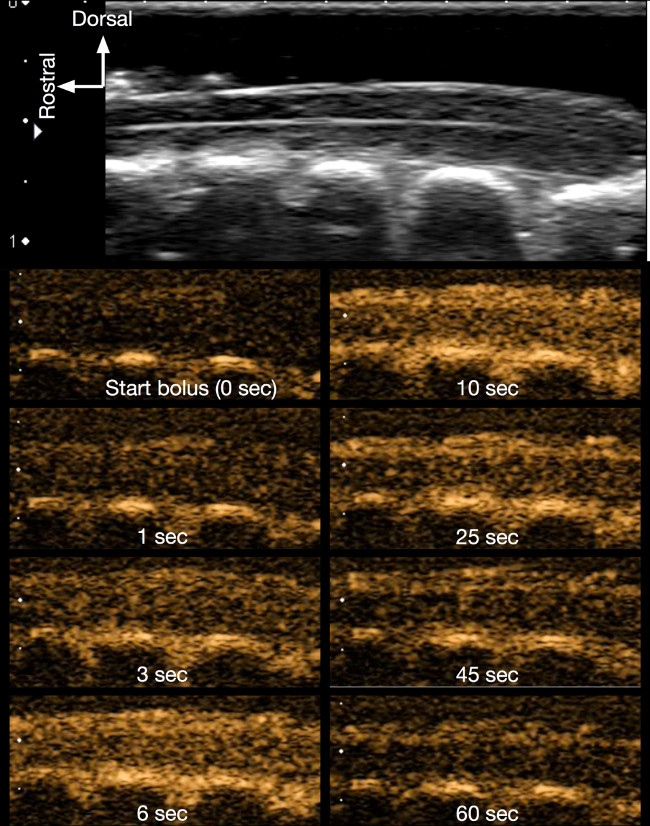
Figure 8. Contrast imaging of the intact spinal cord. The successive figures in contrast mode (orange coloured images) show how the contrast agent (microbubbles) progressively appears following the infusion, thereby enhancing the contrast of the spinal cord. Bolus infusion lasts about 10 sec and the contrast data was recorded for 1 min. Please click here to view a larger version of this figure.
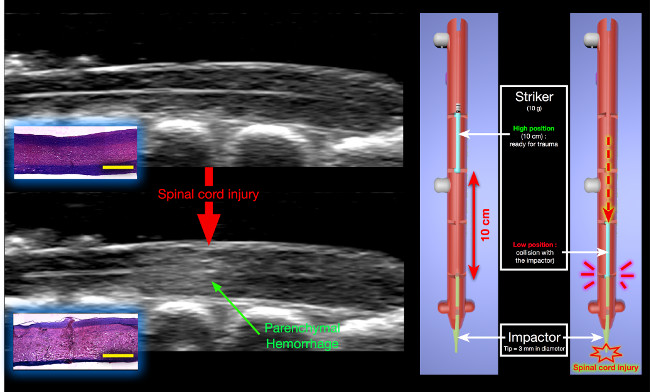
Figure 9. Changes in B-mode following experimental SCI. A hyperechoic lesion appears inside the parenchyma, corresponding to the initial parenchymal hemorrhage post-SCI. Histology (H&E staining) : The hemorrhage results from massive traumatic disruption of small blood vessels leading to blood extravasation in the parenchyma (yellow scale bar = 2,000 μm). The impaction device is shown on the right. The striker is released from a 10 cm height and collides with the impactor that subsequently generates the spinal cord injury. Please click here to view a larger version of this figure.
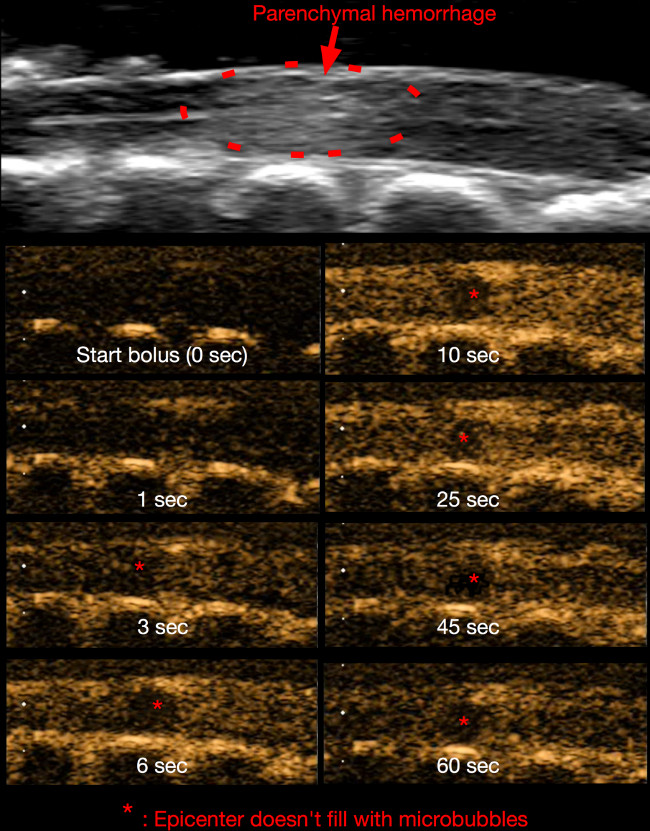
Figure 10. Contrast imaging 15 min post-SCI. Similar to Figure 8, the microbubbles are visible as they pass through the spinal cord microvasculature. At the epicenter (asterisk), the blood flow is obstructed by microvascular disruption. Please click here to view a larger version of this figure.
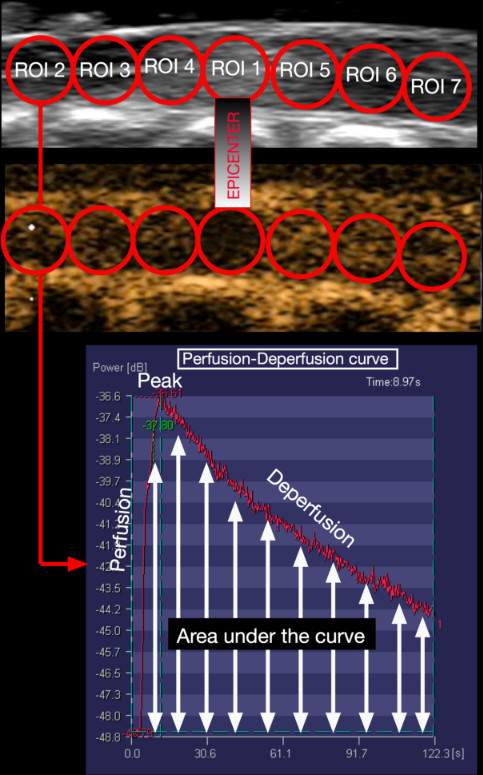
Figure 11. Protocol for SCBF quantification. With Ultra-Extend Software, seven circular and adjacent regions of interest (ROI) are drawn on the longitudinal spinal cord image. The first ROI is placed on the injury epicenter. In each ROI, the software generates a perfusion-deperfusion curve and calculates the area under this curve. This value correlates with the blood flow in this area. Please click here to view a larger version of this figure.
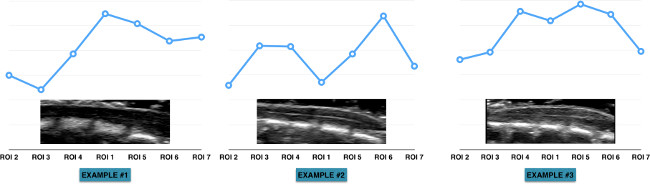
Figure 12. Heterogeneity of the blood flow along the spinal cord. These graphs display the heterogeneity of spinal cord blood flow as well as the variability between animals. This can be largely explained by the vascular anatomy of the spinal cord. However, due to the heterogeneity and variable vascular anatomy, one must use the blood flow measurements (from each ROI) prior to injury as the baseline. The measurements made at the following time-points (post-SCI) are expressed as the percentages change of the baseline. Please click here to view a larger version of this figure.
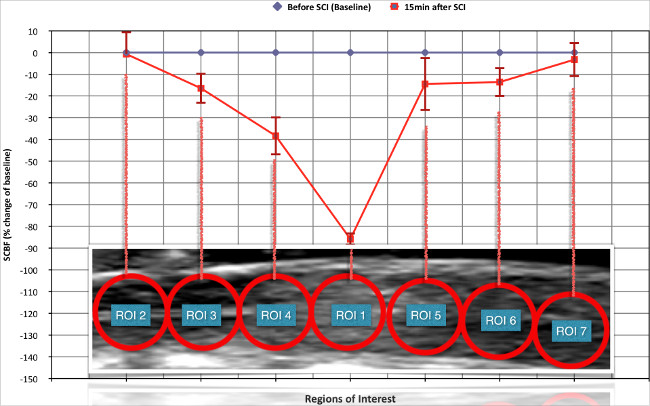
Figure 13. Changes in spinal cord blood flow (SCBF) induced by the experimental spinal cord injury (SCI). 15 min after SCI there is critical ischemia at the level of the epicenter while SCBF remained preserved in the more remote intact areas. In the regions adjacent to the epicenter (both rostral and caudal), SCBF is significantly reduced. This corresponds to the previously described “ischemic penumbra zone”. Please click here to view a larger version of this figure.
