Pressure-volume loop analysis can be used to measure cardiac function in genetically modified mice 14,15 or mice undergoing drug studies16. Representative pressure volume loops are provided from previously published work 16 investigating the effect of ß-Arrestin biased AT1R ligand, TRV120023. To test whether TRV120023 affects cardiac function in vivo, pressure-volume loop analysis was performed on wild type mice receiving conventional and novel angiotensin receptor blockers. Intravenous infusion of TRV120023 increased cardiac contractility significantly (Figure 6 and Table 1, Figure modified from Kim et al. AJP 201216). Contractility measures were derived from aortic constriction.
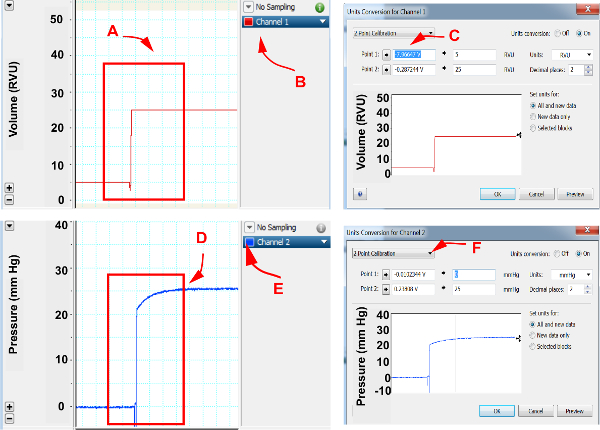
Figure 1. Cardiac pressure and volume calibration. Please click here to view a larger version of this figure.
In pressure volume loop software, assign channels for pressure and volume recordings. (A) Using hemodynamic catheter module, set volume setting to 5 RVU and 25 RVU and select both volumes, (B) Open option under the channel exhibiting volume recordings, (C) Select unit conversion and open “2 point calibration”, select “point 1” and assign as 5 RVU and select “point 2” and assign as 25 RVU , (D) Set pressure to 0 mm Hg and 25 mm Hg, (E) Open options under the channel exhibiting pressure recordings, (F) Select unit conversion and open “2 point calibration”, select “point 1” and assign as 0 mm Hg and select “point 2” and assign as 25 mm Hg. Accept assignments by selecting “OK”.
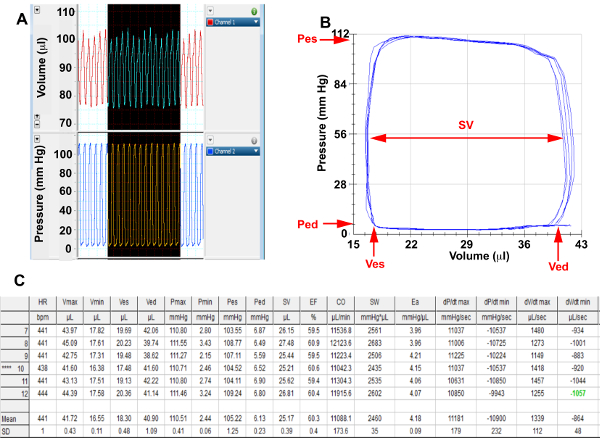
Figure 2. Baseline Hemodynamics Please click here to view a larger version of this figure.
(A) Screenshots from pressure and volume channels of representative cardiac cycles in a basal state, (B) Selected end expiratory baseline pressure-volume loops that have been corrected for parallel conductance for analysis. (C) Baseline hemodynamic summary table calculated from selected loops; Pes, End systolic pressure; Ped, End diastolic pressure; Ves, End systolic volume; Ved, End diastolic volume; SV= Stroke Volume
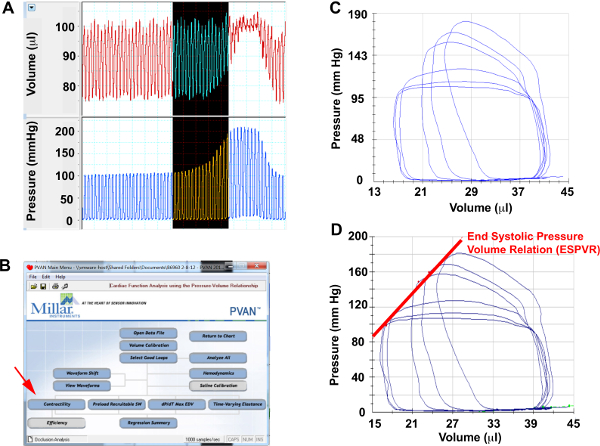
Figure 3. Aortic Constriction Hemodynamics Please click here to view a larger version of this figure.
(A) Screenshots from pressure and volume channels of representative cardiac cycles during aortic constriction, (B) Menu selection to perform contractility analysis, (C) Selected pressure-volume loops during aortic constriction for analysis. (D) ESPVR measured from aortic constriction loops.
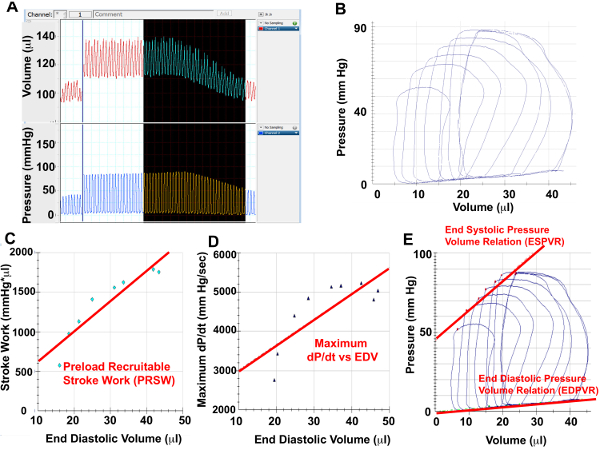
Figure 4. IVC Constriction Hemodynamics Please click here to view a larger version of this figure.
(A) Screenshots from pressure and volume channels of representative cardiac cycles during IVC constriction, (B) Selected pressure-volume loops during IVC constriction for analysis. Using the PV loops from IVC constriction, Preload Recruitable Stroke Work (C), Maximal dP/dt vs EDV (D) as well as ESPVR and EDPVR can be measured.
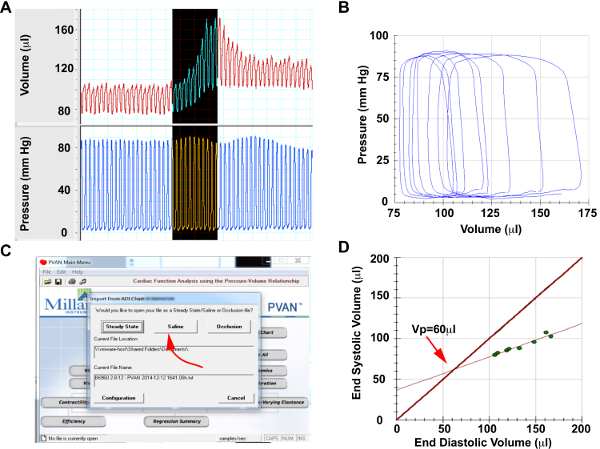
Figure 5. Saline Calibration Please click here to view a larger version of this figure.
(A) Screenshots from pressure and volume channels of representative cardiac cycles during hypertonic saline injection (B) Selected saline injection pressure-volume loops for analysis. Note that pressure will remain constant, while volume will increase significantly, (C) Menu selection to perform saline calibration, (D) Generated lines of measure end-systolic vs end-diastolic volume during saline injection and end-systolic volume=end-diastolic volume. The intersection of these lines provides the parallel conductance of Vp.
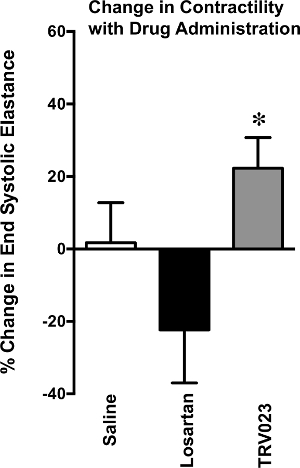
Figure 6. Change in Contractility with Drug Administration
Change in cardiac contractility, measured by end systolic elastance, assessed in wild type mice treated with saline, Losartan 5mg/kg/hr or TRV023 100μg/kg/hr for 5 min. TRV023 treated mice developed a significant increase in end systolic elastance in comparison to Losartan treated mice. *p < 0.05 vs Losartan by 1-way ANOVA.
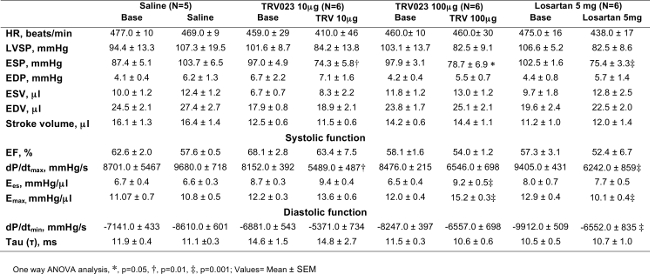
Table 1. Wild type Mice; Hemodynamic Profile in Response of β-arrestin 2 Biased AT1R Agonist
End-systolic pressure (ESP) was decreased significantly after TRV120023 (TRV) and losartan infusion. Cardiac contractility, Ees and Emax was increased significantly in TRV120023 100 μg · kg-1 · min-1 infusion group. (*p < 0.01; †p<0.05; ‡p< 0.001; n=5–6/group). p values reflect comparisons with basal condition within the same treatment group with the use of 1-way ANOVA. Cardiac contractility parameters were derived using an aortic constriction protocol. AT1R, ANG II type 1 receptor; HR, heart rate; EDP, end-diastolic pressure; ESV, end-systolic volume; EDV, end-diastolic volume; Ees, end-systolic elastance; EF, ejection fraction; Emax, maximal elastance; dP/dtmax and dP/dtmin, maximum and minimum rate of pressure change in the ventricle, respectively; τ, isovolumic relaxation constant. Please click here to view a larger version of this table.
