The goal of this image processing procedure is to differentiate the capillaries from the background image so they can be accurately quantified. Both incomplete image processing and excessive image processing are detrimental to the program’s ability to quantify the capillaries. As seen in Figure 3, incomplete image processing makes the capillaries difficult to distinguish from the background. It is critical that the user be able to readily distinguish the border of a capillary since the counting method described above depends on the user’s ability to accurately highlight a few capillaries. On the other hand, as seen in Figure 3, the application of unnecessary image processing steps can lead to blurring of the capillaries and therefore can also be detrimental to the quantification process.
An optimally processed image can be counted within 30 secs and clearly distinguishes capillaries from background as well as individual capillaries from each other. An example of a processed image is seen in Figure 2 part D, with the counted image shown in Figure 3.
Capillary density differs depending on the location of the nailbed being counted. Table 1 shows that capillary density increases with distance from the top row of capillaries at the nailbed. Standardization of the ROI placement is crucial to count reproducibility. Figure 1 shows how images can be altered with different ROI placements.
| ID | T1 | T2 | T3 | T4 | Mean Top | M1 | M2 | M3 | M4 | Mean Middle | L1 | L2 | L3 | L4 | Lowest |
| Patient A | |||||||||||||||
| Baseline | 46 | 45 | 44 | 46 | 45.25 | 64 | 62 | 62 | 62 | 62.5 | 66 | 67 | 66 | 66 | 66.25 |
| Venous Occlusion | 51 | 53 | 49 | 59 | 53 | 59 | 61 | 64 | 69 | 63.25 | 70 | 70 | 75 | 72 | 71.75 |
| Patient B | |||||||||||||||
| Baseline | 47 | 51 | 48 | 51 | 49.25 | 73 | 74 | 75 | 81 | 75.75 | 76 | 85 | 81 | 80 | 80.5 |
| Venous Occlusion | 68 | 57 | 65 | 64 | 63.5 | 75 | 78 | 76 | 72 | 75.25 | 91 | 89 | 93 | 83 | 89 |
| Patient C | |||||||||||||||
| Baseline | 51 | 54 | 51 | 56 | 53 | 66 | 59 | 58 | 60 | 60.75 | 60 | 61 | 62 | 69 | 63 |
| Venous Occlusion | 62 | 66 | 57 | 59 | 61 | 63 | 63 | 73 | 65 | 66 | 83 | 74 | 81 | 77 | 78.75 |
Table 1: Variation in Capillary Counts with Differential Positioning in the Fingernail Bed. This table shows the counts obtained for three different patients (A, B, C) when the ROI box is variably positioned at the top (counts T1 – T4), middle (M1 – M4), and lower regions (L1 – L4) of the fingernail bed. The mean counts increase from the top to lower regions, demonstrating the need for standardization of ROI box placement to compare counts obtained from different laboratories.
Performing counts in the area described in step 1.2, baseline counts should range from 30 to 60 capillaries/mm2 while venous occlusion counts can range anywhere from 50 to 100. As seen in Table 1, these densities differ from other literature. Capillary density counts obtained in the authors’ laboratory are most likely lower because this lab begins counts at the first row of capillaries, where the density is lowest. As seen in Table 1, performing counts in lower regions of the nailbed increase the counts toward values obtained previously by Antonios et al9 and Debbabi et al.16 This discrepancy illustrates the need for standardization in quantification of nailbed capillaroscopy by counting the first (most proximal) row of capillaries. Counting at the first row of capillaries is also optimal because the capillaries are most clearly and completely visualized in the first row and progressively become less visible with subsequent rows.
Blinded reproducibility studies using N = 10 subjects and two independent observers were conducted. Reliability results refer to the average A, B, and C counts, obtained by averaging results across 4 images for each. The A, B, and C counts represent different physiologic states within the same individual that are used to assess microvascular health, briefly summarized here. Details have been previously published 21. Capillary Density is defined as the number of capillaries per square millimeter (mm2) of finger nailfold skin. Stage A is a resting baseline stage where the capillaries are continuously perfused 16. Stage B occurs during postocclusive reactive hyperemia. These counts represent the sum of continuously perfused and intermittently perfused (functional reserve) capillaries. This stage is used as a measure of capillary function 16.
Stage C occurs during venous occlusion, therefore showing maximal capillary density including both perfused (with active red blood cell (RBC) motion) and nonperfused (filled with stagnant, non-moving RBCs) capillaries.22
For intra-rater reliability, the intraclass correlations (ICC) were 0.93 for mean A counts, 0.93 for mean B counts, and 0.94 for mean C counts. For inter-rater reliability, the ICCs were 0.94 for mean A counts, 0.98 for mean B counts, and 0.94 for mean C counts. Accordingly, the technique described here demonstrates excellent reliability with good results for both intra and inter-observer reproducibility.
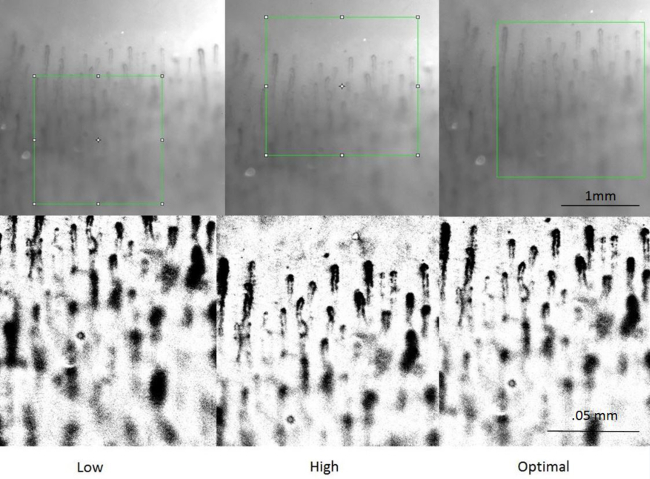
Figure 1. Standardizing the Crop Location. This figure illustrates how variable placement of the ROI box visibly alters the cropped image. On the left, the box is placed too low, cutting off the first row of capillaries. The middle box is placed too high, causing a blank space above the first row of capillaries. The box on the right is optimally placed. Its cropped image shows the first row of capillaries at the very top of the image. Please click here to view a larger version of this figure.
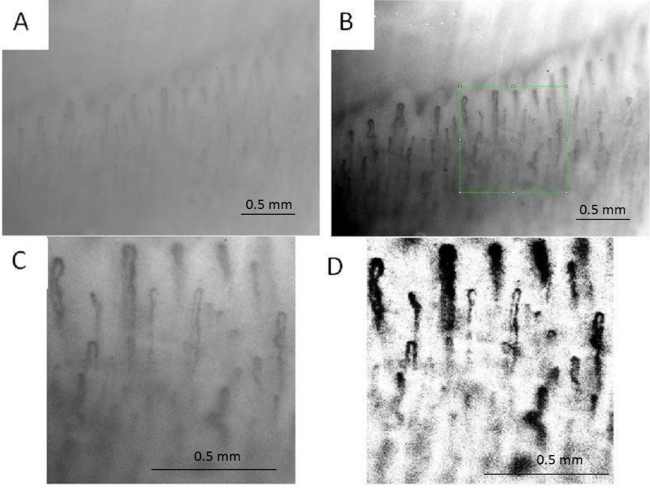
Figure 2. Stages of Image Processing.(A) Stage A shows the initial image taken from the subject’s nailbed with a monochrome camera; (B) Stage B shows the original image after the first contrast enhancement. The green box shows a 530 x 530 pixel box, which is equivalent to 1 x 1 mm box for the camera; (C) Stage C represents the 1 mm box cropped from image B; (D) Stage D shows the enhanced image after applying the enhancements discussed above. Please click here to view a larger version of this figure.
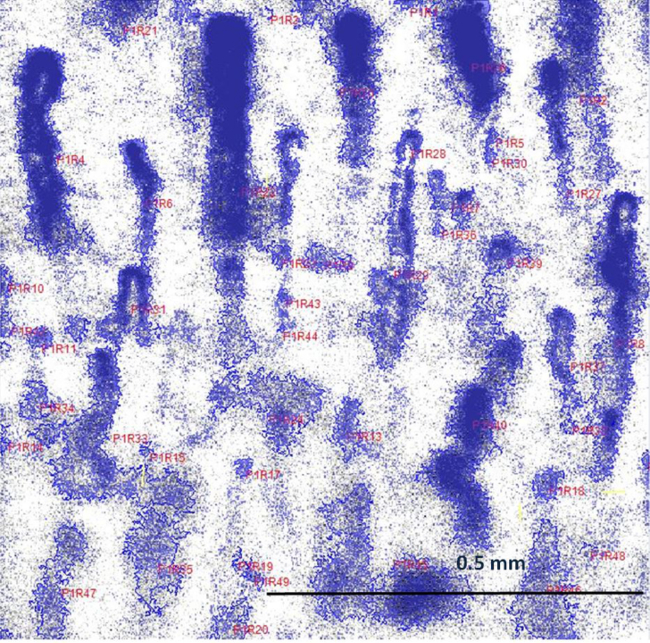
Figure 3. Final Counted Image. The enhanced, counted image. The total count determined for this image was 54 capillaries/mm2. Please click here to view a larger version of this figure.
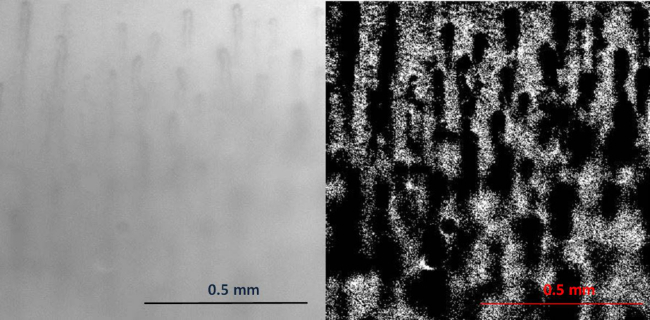
Figure 4. Improper Image Processing. Please click here to view a larger version of this figure.
The photo on the left shows a photo that is not processed enough. The capillaries are difficult to distinguish from the background and the quantitation process will be negatively affected. The photo on the right shows the same image after incorrect image processing. Individual capillaries are difficult to distinguish from their neighbors and thus the quantitation process will be negatively affected.
