There are different rat and mouse models to satisfy the needs of different epilepsy types. To induce focal TLE, 0.5 µL of pilocarpine (2.4 mg/µL) is administered into the left CeA. The predominant epileptiform ECoGs are acquired from the ECoG electrode on the parietal lobe of the left hemisphere (Figure 1A: b), and rare epileptic activities are picked up from the rest of the ECoG electrodes (Figure 1A: a, c, d, e, and f) when the pilocarpine is administered. Epileptiform ECoGs are primarily recorded immediately after pilocarpine administration. These results are adopted from 8. These results indicate the successful induction of focal TLE in rats after the direct injection of low-dose pilocarpine into the CeA.
Within 5 min, the IP injection of 300 mg/kg pilocarpine induces severe cholinergic effects on behavior, such as piloerection, salivation, red eyes, shivering, and facial automatisms. The severity of these behavioral signs gradually increases until an ECoG generalized seizure occurs (Figure 1B, blue box). SE also occurs following the generalized epilepsy (Figure 1B, red box). These results are adopted from13. Our results suggest that an IP injection of 300 mg/kg pilocarpine is a reliable method to induce ECoG-documented generalized epilepsy and SE. However, the survival rate after SE development is between 15% and 20%. The PTZ-kindling model of epilepsy in mice is used to develop spontaneously and recurrently generalized epilepsy. PTZ at a dose of 0.035 mg/g mouse bodyweight is IP injected at a particular ZT point (e.g., the beginning of the dark period, ZT13) every other day, and each injection is separated by a one-day interval. There are no epileptiform ECoGs found during the dark period after the 1st injection of PTZ (Figure 1C: a) or during the following dark period, when it is an off day for injection (Figure 1C: b). No significant epileptic activity is found after the 2nd, 3rd, and 4th injections (data not shown here). However, epileptiform ECoGs are induced after the 5th PTZ injection (Figure 1C: c and d), along with spontaneously and recurrently generalized epilepsy (Figure 1C: e and a').
We classified vigilance states into wakefulness, NREM sleep, and REM sleep according to the criteria we mentioned in the protocol. Wakefulness is visually scored by desynchronized ECoGs with low amplitude and high frequency. The power density values in the delta frequency band (0.5 – 4 Hz) are generally greater than those in the theta frequency band (6 – 9 Hz) during wakefulness, and more high frequency spectra (> 10 Hz) are found. Wakefulness exhibits a high amplitude of EMG and lots of locomotor activity. Furthermore, cortical temperature gradually increases when the vigilance state transits from either NREM sleep or REM sleep to wakefulness (Figure 2). NREM sleep is characterized by synchronized ECoGs with high amplitude and low frequency. The power density values are dominant in the delta frequency band. The EMG amplitude gradually declines, and no locomotor activity is exhibited during NREM sleep. Cortical temperature decreases when the vigilance state transits from wakefulness into NREM sleep (Figure 2). During REM sleep, the ECoG wave is desynchronized, the amplitude is reduced, the predominant EEG power density occurs within the theta frequency (6.0 – 9.0 Hz), EMG activity is the lowest, phasic body twitch is observed, and cortical temperature rapidly increases (Figure 2).
We demonstrated the distinct effects of EA on epileptic activity when EA stimulates the Fengchi acupoints with either a high-frequency stimulation (100 Hz) or a low-frequency stimulation (10 Hz). In Figure 3A, a microinjection of 0.5 µL of pilocarpine (2.4 mg/µL) into the left CeA induces focal TLE, as mentioned previously (B). However, 100-Hz EA of bilateral Fengchi acupoints exacerbates the pilocarpine-induced epileptiform ECoGs (C). These results are adapted from 8. In contrast, 10-Hz EA of bilateral Fengchi suppresses the pilocarpine-induced epileptiform ECoGs (Figure 3B: C). These results are adapted from 7. Administration of pilocarpine into the left CeA also suppresses NREM sleep during the light period of the 12-h light:dark cycle (Figure 4A & 4B). The reduction of NREM sleep during a few hours of the dark period is primarily due to the effect of anesthesia, and is not a direct effect of EA15. Application of 100-Hz EA further deteriorates the pilocarpine-induced suppression of NREM sleep (Figure 4A). In contrast, a 10-Hz EA of bilateral Fengchi acupoints increases NREM sleep per se during the dark period and blocks the pilocarpine-induced reduction of NREM sleep during the light period (Figure 4B). These results are adopted from 9.
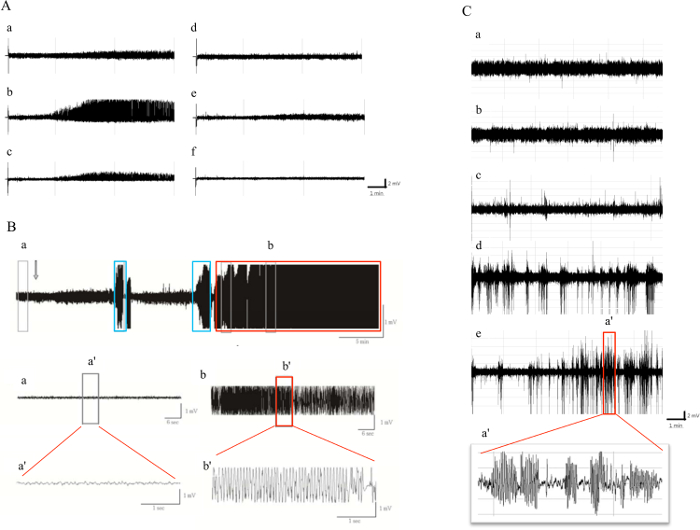
Figure 1: Different Epilepsy Models in Rats and Mice. A demonstrates the focal TLE in rats. B elucidates the generalized epilepsy with SE in rats. C indicates the spontaneous and recurrent epileptiform ECoGs. (A) (a), (b), (c), (d), (e), and (f) represent the ECoG signals recorded from the electrodes placed on the left frontal, left parietal, left occipital, right frontal, right parietal, and right occipital cortices, respectively. (B) The arrow indicates the IP injection of pilocarpine. The grey box (a) demonstrates the baseline ECoGs obtained before the pilocarpine injection. The blue box shows the epileptiform ECoGs of generalized epilepsy. The red box (b) represents the SE. The ECoG signals extracted from (a) and (b) are shown in (a') and (b'). (C) (a) represents the ECoGs acquired after the 1st PTZ injection and (b) represents the ECoGs recorded the day after the 1st PTZ injection in mice. Epileptic activities occur after the 5th PTZ injection (c) and afterwards. The recurrent epileptic ECoGs that occur the day after 5th PTZ injection are shown in (d). The recurrent epileptic ECoGs recorded 5 days after the 5th PTZ injection are shown in (e). The figure at the bottom (a') represents the ECoGs extracted from the red box. Please click here to view a larger version of this figure.
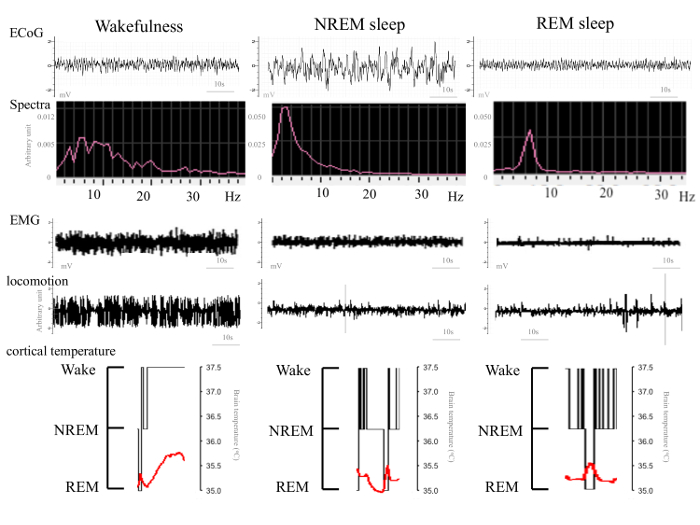
Figure 2: Classification of Vigilance States: Wakefulness, NREM Sleep, and REM Sleep. The vigilance states of rats are classified by the parameters from the ECoGs, ECoG spectra, EMGs, locomotor activity, and cortical temperature. The vigilance states of mice are characterized by the same parameters, except cortical temperature is not applicable.
Please click here to view a larger version of this figure.
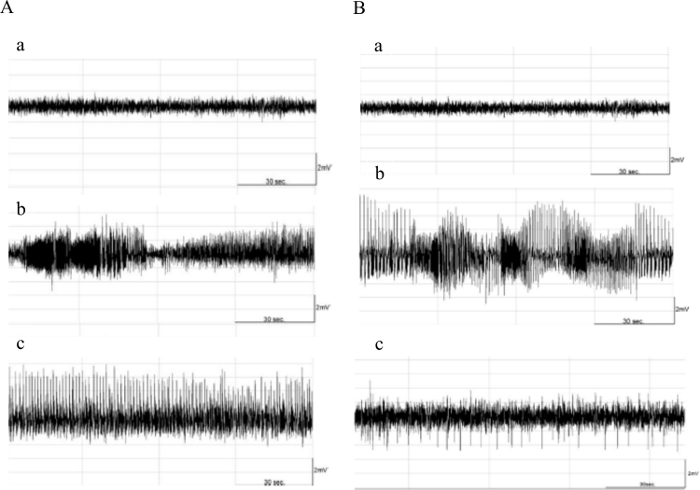
Figure 3: The Effects of 100-Hz and 10-Hz EA on Epilepsy. In (A), the first ECoG trace demonstrates the baseline ECoGs (a). Microinjection of pilocarpine into the left CeA induces focal TLE (b). Application of 100-Hz EA at bilateral Fengchi acupoints exacerbates the epileptiform ECoGs (c). In (B), the first ECoG trace demonstrates the baseline ECoGs (a). The microinjection of pilocarpine into the left CeA induces focal TLE (b). The application of 10-Hz EA at bilateral Fengchi acupoints suppresses the epileptiform ECoGs (c). Please click here to view a larger version of this figure.
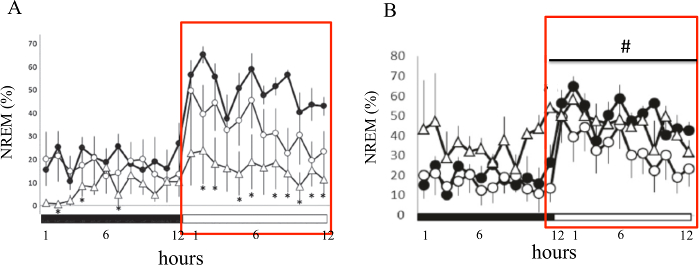
Figure 4: The Effects of 100-Hz and 10-Hz EA on Epilepsy-induced Sleep Disruptions. (A) Focal TLE induced by the microinjection of pilocarpine into the left CeA reduces NREM sleep during the light period. 100-Hz EA further deteriorates the epilepsy-induced sleep disturbance. (B) The application of 10-Hz EA blocks the epilepsy-induced reduction of NREM sleep during the light period. Furthermore, 10-Hz EA enhances NREM sleep during the dark period. Values are represented as mean ± SEM. The black circle represents the values obtained before the microinjection of pilocarpine, the open circle depicts the data acquired after the pilocarpine injection, and the open triangle demonstrates the values obtained after EA stimuli. The black bar represents the dark period of the 12-h light:dark cycle, and the white bar depicts the light period. * represents the statistical difference between the 100-Hz EA + pilocarpine group and the control (ANOVA, P < 0.05) and # indicates the statistical difference between the 10-Hz EA + pilocarpine group and the pilocarpine group (ANOVA, p < 0.05). Please click here to view a larger version of this figure.
