The culture of ADSCs and the procedure to obtain the ADSC sheet is shown in Figure 1. Figure 2 shows the construction of the graft, composed of two ADSC sheets layered upon each other on their paper support membrane. ADSCs were previously labeled with the PKH67 fluorophore to allow in vivo graft monitoring with pCLE. Figure 3 shows the different steps of extended esophageal endoscopic submucosal dissection, resulting in a 5-cm and hemi-circumferential esophageal scar. Figure 4 shows the endoscopic transplantation procedure. The transplantation was successful for all animals after 10 min of gentle application. Figure 5 shows the positive pCLE evaluation on day 3, confirming the success of the transplantation procedure.
The follow-up period allowed for multimodal stricture analysis. The different assessments are showed in the following figures and table. Compared to control animals, the transplanted animal group showed less frequent alimentary trouble and greater weight gain on day 28. One animal from the transplanted group developed a severe esophageal stricture compared to all animals in the control group. Compared to transplanted animals, control animals developed significant fibrotic tissue. Table 1 shows clinical and endoscopical findings during the follow-up period. Figure 6 shows the endoscopic and radiological findings at the end of the follow-up period in transplanted and non-transplanted animals. Figure 7 shows the different histological findings between transplanted and control animals. These data confirm the effectiveness of ADSC-sheet transplantation for esophageal stricture prevention.
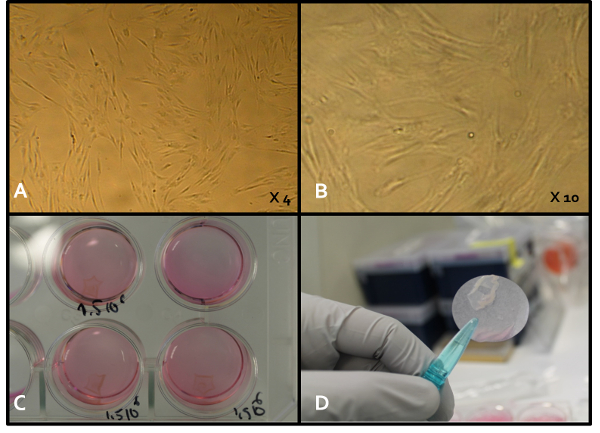
Figure 1. ADSC-sheet Construct. A and B. Early-passage ADSCs in standard culture dishes with different magnifications. ADSC sheets were obtained by culturing PKH-labeled ADSCs on commercial temperature-responsive culture dishes. C. When the incubation temperature was reduced to 20 °C (room temperature), all cells spontaneously detached from the dish surfaces as intact ADSC sheets, without the need for enzymatic treatment. D. An ADSC sheet harvested before graft construction using a transfer membrane. Please click here to view a larger version of this figure.
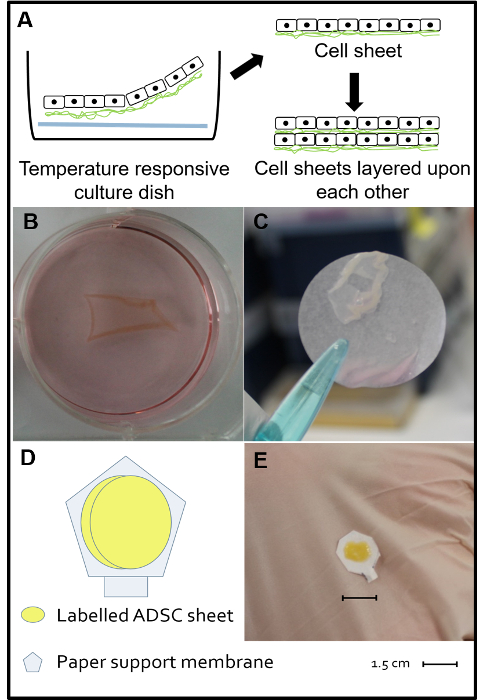
Figure 2. Double ADSC-sheet Construct. A, B, and C. The day before transplantation, PKH-labeled ADSCs were harvested at early passage number (P4 – P5), seeded on a 12-well temperature-responsive cell culture, and cultured at 37 °C and 5% CO2 with alpha minimum essential medium including 10% fetal veal serum and 1% antibiotics (penicillin and streptomycin). Each well was coated with a poly-N-isopropylacrylamide membrane (at the bottom of each well) and seeded with 1.5 x 106 cells. When the incubation temperature was reduced to 20 °C (room temperature), all cells spontaneously detached as intact ADSC sheets without the need for enzymatic treatment. D. Theoretical schema of the double cell-sheet construct composed of two ADSC sheets layered upon each other and applied to a paper support membrane. E. Macroscopic view of a completed double cell-sheet construct. Modified from Reference 15. Please click here to view a larger version of this figure.
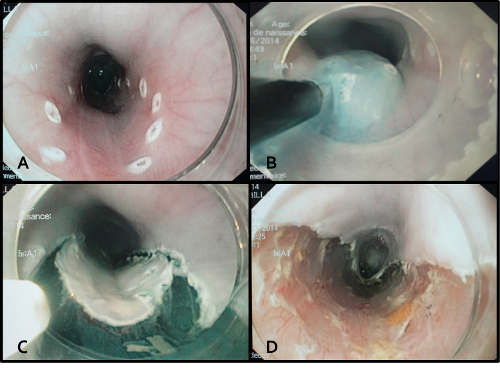
Figure 3. Endoscopic Submucosal Dissection Procedure. A. Endoscopic marks were created to delineate the resection area, ranging from 40 to 45 cm from the dental arch and involving half of the circumference. B. The submucosal injection of a glycerol solution containing indigo carmine dye. The goal of this injection was to separate the mucosal layer from the muscular layer in order to expose the submucosal layer. C. Peripheral incisions were performed externally to the endoscopic marks, revealing the injected submucosal layer. D. The endoscopic view at the end of the submucosal dissection showing a 5 cm-long and hemi-circumferential esophageal scar. Please click here to view a larger version of this figure.
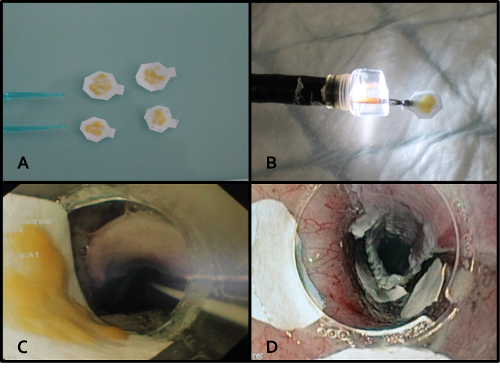
Figure 4. Double ADSC-sheet Endoscopic Transplantation Procedure. A. Four ADSC constructs ready to be transplanted. B. Protection of the ADSC construct under a large endoscopic cap before transplantation. C. Endoscopic view of the crossing of the animal pharynx, showing the ADSC construct protected under the endoscopic cap. D. 10 min of application was sufficient to obtain sheet adherence. Application was performed using the endoscopic cap or endoscopic forceps. Please click here to view a larger version of this figure.
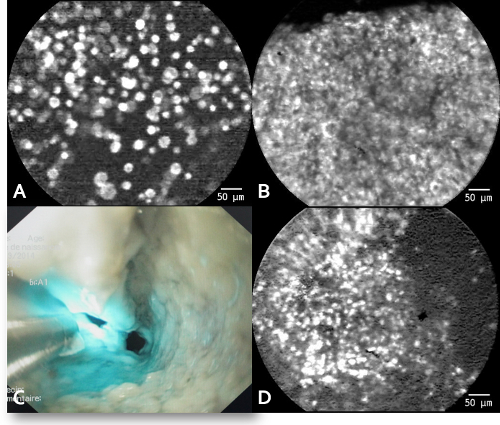
Figure 5. pCLE Findings. pCLE on day 3 shows spontaneous and intense signals similar to those obtained in vitro, compatible with a successful cell-sheet transplantation. No signal was found on days 14 and 28. A. The in vitro pCLE signal of ADSCs in suspension. B. The in vitro pCLE signal of ADSCs organized in a cell sheet. C. The in vivo pCLE probe application to the esophageal scar. D. The in vivo pCLE signal of ADSCs visualized on day 3 after transplantation. Modified from Reference 15. Please click here to view a larger version of this figure.
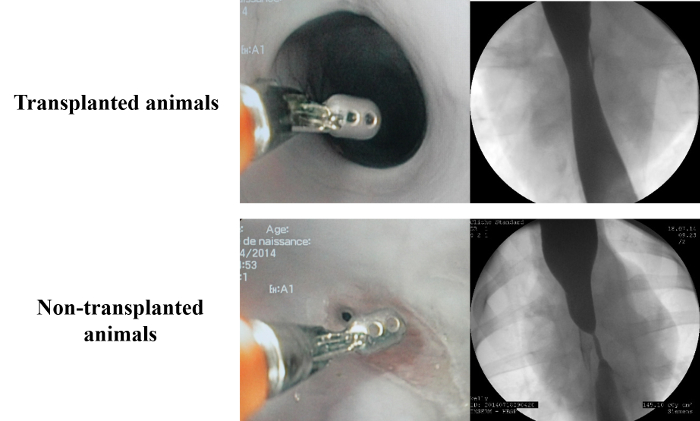
Figure 6. Results of the Morphological Analysis on Day 28. Compared to the control group, the endoscopic and radiological findings on day 28 showed a short and light stricture without upstream dilatation and a completely re-epithelialized mucosa. Modified from Reference 15. Please click here to view a larger version of this figure.
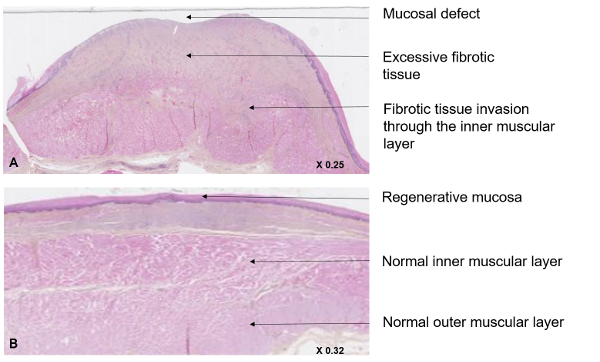
Figure 7. Histological Evaluation of the Stricture Areas. The histological analysis was performed after HES-labeling and slide digitalization. In transplanted animals (A), the healing process was improved, with increased re-epithelialization and decreased fibrosis development, compared to non-transplanted animals (B). Intense fibrotic tissue development was observed due to muscularis mucosae destruction, fibrotic inner muscularis layer invasion, and large mucosal defects. Modified from Reference 15. Please click here to view a larger version of this figure.
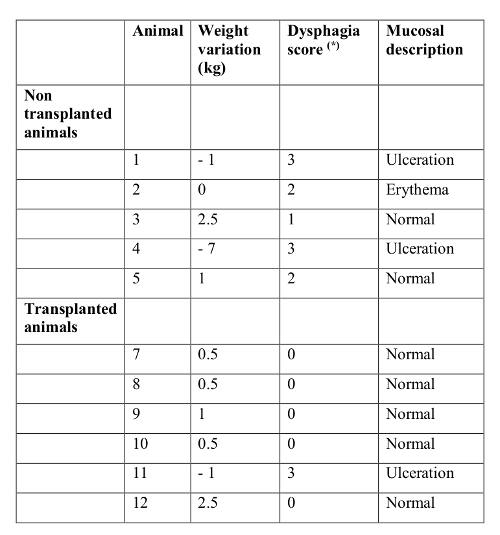
Table 1. Clinical Assessments during the Follow-up Period. Clinical assessments were performed using a daily clinical evaluation according to the Mellow Pinkas score and with weight variation. (*) Mellow Pinkas score16. Modified from Reference 15.
