Summary
This curriculum outlines how to execute a simulation-based boot camp to teach providers how to manage mechanically ventilated patients.
Abstract
Medical management of mechanically ventilated patients is challenging to novice providers. Incorrect management of this population may lead to increased morbidity and mortality. A three-day simulation-based boot camp serves to provide one-on-one instruction with a critical care provider. These intensivists may dispense personalized immediate feedback as learners engage in hands-on practice with a real mechanical ventilator. Multiple different pathologies can be reviewed that may not be encountered in the clinical setting. Learners can visualize immediate consequences of their actions and may troubleshoot and ask questions, all while in a safe learning environment. We describe the use of human-patient simulators connected to breathing simulators and mechanical ventilators. Potential curriculum executors should be aware of the cost of the equipment and the time needed to dedicate to boot camp execution; however, this intensive interactive training has been shown to increase provider competency, knowledge, and confidence in ventilator management. This curriculum outline provides guidance on how to execute a simulation-based boot camp to train providers on the management of mechanically ventilated patients.
Introduction
This boot camp was developed to teach residents how to manage a mechanically-ventilated patient, as well as troubleshoot ventilator alarms. Management of this patient population may be intimidating to the novice practitioner who may have limited experience with critically ill patients. Teaching critical care principles at the bedside is made more difficult by national work-hour restrictions1,2, and medicolegal concerns3 in the United States. Simulation is an effective modality to develop and refine critical care skills4,5, as well as invasive procedures6,7,8,9,10. Through simulation, learners may experience what the consequences of their medical decision-making is without putting patients at risk. This curriculum allows for a variety of different learning modalities, including bedside teaching from an intensivist, hands-on practice with a ventilator, and supplemental asynchronous reading.
Previous studies have shown increased knowledge with mannequin-based education of mechanical ventilation11,12. Spadaro et al.11 compared computer-based training with mannequin-based training for anesthesiology residents undergoing simulation-based teaching of mechanical ventilation. Residents who underwent mannequin-based training had higher key action and global rating scores. As noted in our previous study12, first-year residents demonstrated improved knowledge, confidence, and competency after the conclusion of this boot camp curriculum.
As written, this three-day curriculum allows for educators to initially assess their learners' baseline knowledge on day one, as well as evaluate changes in competency, knowledge, and confidence upon curriculum completion on day three. Days one and three are dedicated towards assessment, while the second day is focused on bedside teaching by content experts. Pathological conditions (acute respiratory distress syndrome [ARDS], atelectasis secondary to mucus plugging, and pneumothorax) were used for the initial assessment and final testing days, while an altered mental status station was added during the teaching day to review ventilator basics. Dynamic hyperinflation was also added to the teaching day as to reinforce ventilator diagnostics and management, including its consideration in patients with a high plateau pressure. Educators may substitute the pathologies as they feel appropriate for their teaching needs.
In preparation, simulation faculty held an initial rehearsal day to ensure all participating educators were aware of their roles and to ensure equipment was working appropriately. While we used simulation faculty for assessment and critical care physicians for teaching, educators may adjust the roles of faculty as resources dictate. Execution of this boot camp requires preparatory logistics planning. First-year residents should be scheduled protected time to ensure they can complete all three days of the curriculum. Intensivists will need to schedule time off in advance to attend bedside teaching sessions. Simulation equipment such as breathing simulators, mechanical ventilators, and human-patient simulators may have to be purchased, rented, or borrowed.
Protocol
All methods described here were found to be exempt from review by the Summa Institutional Review Board.
1. Day 1 – Pre-Testing Evaluation
- Print critical action checklists, pretest confidence surveys, pretest cognitive multiple-choice exams.
- Place three human-patient simulators in ICU beds with the following designations: acute respiratory distress syndrome (ARDS), complete lung atelectasis secondary to mucus plugging, and pneumothorax. Set simulators in separate rooms or far enough apart that learners will not be able to easily hear the other simultaneously executed sessions. Place simulators in a dedicated learning space.
- Intubate the human-patient simulators. Do not place the endotracheal tube in the trachea of the simulator, but rather through a hole in the simulator's inner cheek that leads to the back of the simulator's neck.
- Connect the corrugated airway tubing from the lung simulator to the endotracheal tube that is now hidden behind the simulator's neck. Once connected, the lung simulator is now functional. Use a pillow to conceal this connection.
- Turn on the lung simulator. Choose selected pathologic state from the menu in the patient library folder. Initiate the selected pathology on the lung simulator.
- Connect the mechanical ventilator to the endotracheal tube coming out of the simulator's mouth. If the ventilator is connected to the endotracheal tube prior to initiating the lung pathology software program, the ventilator will not function properly.
- Connect human-patient simulators to breathing simulators. Connect the intubated human-patient simulators to mechanical ventilators.
- Place a simulated patient monitor by each human-patient simulator. Select the vital sign software within the lung simulator program. Choose appropriate initial vital signs for onset of simulated patient presentation. Enable the vital signs monitor.
- Upload pre-selected patient's vital signs, portable chest X-ray images, electrocardiograms, and arterial blood gas measurements for each patient case to each respective patient monitor (e.g., autoPEEP images are uploaded to the human-patient simulator designated as the autoPEEP patient).
- Set out critical actions checklists at each station for each learner wherever faculty members will be observing the case. This may be behind a one-way glass or on a bedside table, but at enough distance away that the learners will not be able to read the checklists. Assign one faculty member to each station.
- Have each learner pick a four-digit identifying code to use for confidence surveys, cognitive exams, and critical action checklists. The codes may be used to review collected data in an anonymous fashion. Learners may choose any four-digit code that they will consistently remember throughout the curriculum.
- In a separate room, administer 5-minute pretest confidence survey to learners. Upon its completion, administer 25-minute pretest cognitive multiple-choice exams to learners.
- Have learners report to a station, with one learner present at each station. Remaining students may wait in a separate room. Have learners provide their four-digit identifying code to faculty for their critical action checklist.
- Have faculty read the case stem to learner. Allow learners a maximum of ten minutes per station to work through a scenario. Do not administer feedback during case. At the conclusion of the scenario, dismiss learners to return back to their separate room.
- Have faculty fill out critical action checklists for each learner upon completion of each case. Rotate learners through all stations individually until all learners have completed all stations. Distribute supplemental readings to learners via paper or email.
2. Day 2 – Curriculum and Educational Intervention
- Set up five stations with human-patient simulators, breathing simulators, ventilators, and monitors as described above.
- Assign each station one of the following topics: ARDS, atelectasis secondary to mucus plugging, pneumothorax, altered mental status secondary to drug overdose, and dynamic hyperinflation. Arrange learners in groups of two or three people. Assign one faculty member to each station.
- Allow each team 10 min to work through a case scenario. Give faculty 35 min to provide feedback and bedside instruction. Rotate learners through the remaining four stations.
3. Day 3 – Post-testing Evaluation
- Print critical action checklists, posttest confidence surveys, post-test cognitive multiple-choice exams. Set up three stations with human-patient simulators, breathing simulators, ventilators, and monitors as described above. Assign each station one of the following topics: ARDS, atelectasis secondary to mucus plugging, pneumothorax.
- Upload vital signs, portable chest X-ray images, electrocardiograms, and arterial blood gas measurements for each patient case to each respective patient monitor (e.g., autoPEEP images are uploaded to the human-patient simulator designated as the autoPEEP patient).
- Set out critical actions checklists at each station for each learner. Assign one faculty member to each station. Administer 5-minute post-test confidence survey and 25-minute posttest cognitive multiple-choice exam.
- Have learners report to a station, with one learner present at each station. Remaining students may wait in a separate room. Have learners provide their four-digit identifying code to faculty for their critical action checklist.
- Have faculty read the case stem to learner. Allow learners a maximum of ten minutes per station to work through a scenario. Do not administer feedback during case. At the conclusion of the scenario, dismiss learners to return back to their separate room.
- Have faculty fill out critical action checklists for each learner upon completion of each case. Rotate learners through all stations individually until all learners have completed all stations. Administer 10-minute post-curriculum survey to all learners.
Representative Results
As noted in Yee et al, first-year residents who underwent this boot camp demonstrated significantly improved confidence, knowledge, and performance12. Cognitive knowledge, assessed by the pre- and post-intervention multiple choice tests, increased from a mean score of 40.3% to 67.1%, with a mean change in score of +26.8% (Figure 1).
Critical actions were evaluated by faculty on days 1 and 3. The ARDS case had an initial mean of 1.5 critical actions met on day 1 (out of a total of 5), which increased to 4.1 on day 3. The atelectasis secondary to mucus plugging case had an initial mean of 1.24 on day 1 (out of a total of 5) and a postintervention score of 4.47 on day 3 (Figure 2).
Learners felt more confident after the boot camp intervention. Their initial confidence on day 1 was rated as a mean score of 1.56 out of 5, which increased to a mean score of 3.64 on day 3 (Figure 3).
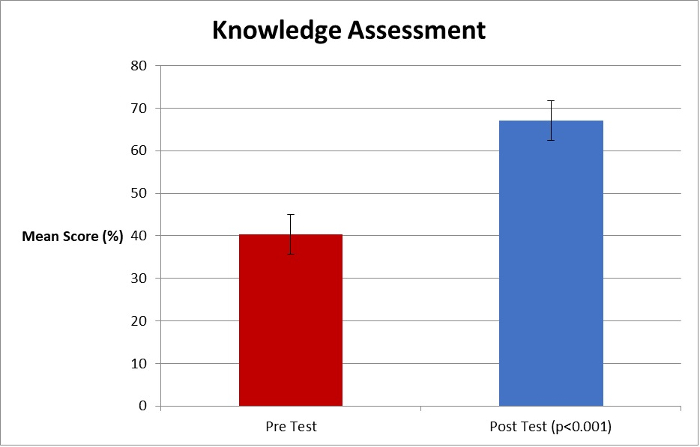
Figure 1: Knowledge Assessment Pre- and Post-Intervention
This figure has been reformatted with permission from Yee J. et al. Mechanical Ventilation Boot Camp: A Simulation-Based Pilot Study. Crit Care Res Pract. 2016, (2016). doi:10.1155/2016/4670672. Please click here to view a larger version of this figure.
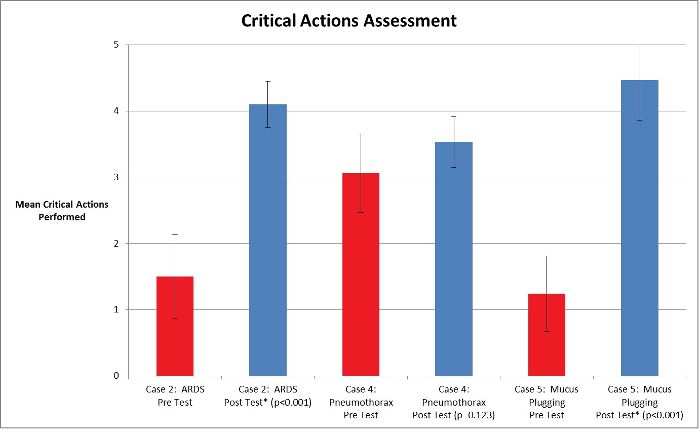
Figure 2: Critical Actions Performance Assessment Pre-and Post-Intervention
This figure has been reformatted with permission from Yee J. et al. Mechanical Ventilation Boot Camp: A Simulation-Based Pilot Study. Crit Care Res Pract. 2016, (2016). doi:10.1155/2016/4670672. Please click here to view a larger version of this figure.
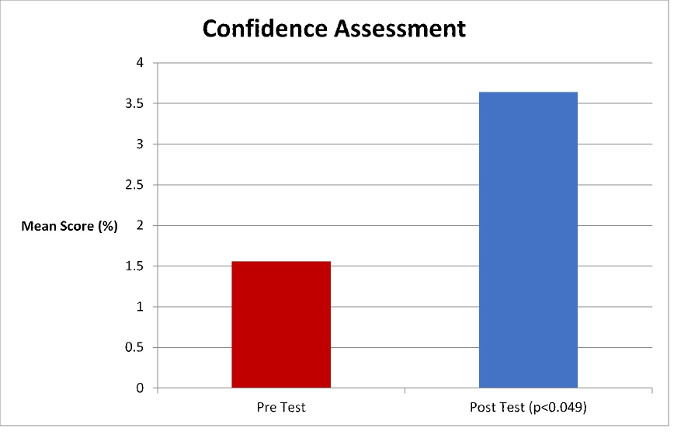
Figure 3: Confidence Assessment Pre- and Post-Intervention
This figure has been reformatted with permission from Yee J. et al. Mechanical Ventilation Boot Camp: A Simulation-Based Pilot Study. Crit Care Res Pract. 2016, (2016). doi:10.1155/2016/4670672. Please click here to view a larger version of this figure.
Discussion
The boot camp consists of three separate sessions. During the first day, learners complete a pre-testing confidence survey and medical knowledge test before undergoing a five-minute scenario. Faculty evaluate the learners using pre-determined critical actions. Leaners are then given asynchronous reading to complete before day 2. The second day is composed of the intervention stage, where groups of 2-3 learners work through five different scenarios. Faculty are at the bedside to provide immediate and personalized feedback. The third day is the post-testing evaluation, where learners complete a post-testing confidence survey and medical knowledge test. They then undergo a five-minute scenario, rated against critical actions.
In the authors' opinion, the most critical point of the curriculum is the bedside teaching by critical care content experts. As reviewed in the literature, the debriefing process is the most important step in simulation and is essential for knowledge gains.13,14
The curriculum evolved throughout its execution. Residents were invited to provide feedback at the end of the curriculum. Many residents expressed a desire to review articles that provided foundational knowledge of an overview of mechanical ventilation and pulmonary physiology. Faculty also became more streamlined in their teaching presentations as the curriculum developed.
Limitations are largely related to finances and time. Renting or purchasing simulation equipment may be expensive, particularly if a simulation center does not regularly use this sophisticated simulation equipment. Training simulation staff to become readily proficient on the use of the breathing simulators required a significant amount of time. Intensivists had to schedule time off well in advance to be available for teaching. We suggest that interested educators dedicate ample time to ensure they have sufficient funding and time to execute this curriculum.
There is a paucity of literature describing simulation as a method to teach novice learners the principles of ventilator management. Learners are able to manage low-frequency events on mannequins versus learning on critically-ill patients. This curriculum provides a means for novice medical providers to visualize the consequences of their management decisions in real-time. The breathing simulators used in conjunction with the mechanical ventilators allow for learners to practice on real clinical equipment for hands-on experience that may be intimidating to use in the clinical setting. Additionally, the curriculum allows for bedside personalized teaching by critical care faculty.
Declarações
The authors have nothing to disclose.
Acknowledgements
The authors would like to thank Anna Ciullo, M.D. for her assistance with curriculum development and execution. There was no outside funding for this report.
Materials
| Puritan Bennett 840 Ventilator | Medtronic | 4-840120EMC-01 | http://www.medtronic.com/covidien/en-us/products/acute-care-ventilation/puritan-bennett-pb840-ventilator.html |
| ASL 5000 Breathing Simulator | IngMar | 31 00 117 | https://www.ingmarmed.com/ |
| Smart Stat Basic | Simulaids | 101-8002 | https://www.simulaids.com/product/101-8002 |
Referências
- Slutsky, A. S. History of mechanical ventilation. From vesalius to ventilator-induced lung injury. Am J Respir Crit Care Med. 191 (10), 1106-1115 (2015).
- Ahmed, N., Devitt, K. S., Keshet, I., et al. A Systematic Review of the Effects of Resident Duty Hour Restrictions in Surgery. Ann Surg. 259 (6), 1041-1053 (2014).
- Ziv, A., Wolpe, P. R., Small, S. D., Glick, S. Simulation-Based Medical Education: An Ethical Imperative. Acad Med. 78 (8), 783-788 (2003).
- Duwat, A., Hubert, V., Deransy, R., Dupont, H. Difficult airway management: assessment of knowledge and experience in anaesthesiology residents. Ann Fr Anesth Reanim. 32 (40), 231-234 (2013).
- Lee, M. O., Brown, L. L., Bender, J., Machan, J. T., Overly, F. L. A medical simulation-based educational intervention for emergency medicine residents in neonatal resuscitation. Acad Emerg Med. 19 (5), 577-585 (2012).
- Barsuk, J. H., Cohen, E. R., Caprio, T., McGaghie, W. C., Simuni, T., Wayne, D. B. Simulation-based education with mastery learning improves residents’ lumbar puncture skills. Neurology. 79 (2), 132-137 (2012).
- Barsuk, J. H., Cohen, E. R., Vozenilek, J. A., et al. Simulation-based education with mastery learning improves paracentesis skills. J Grad Med Educ. 4 (1), 23-27 (2012).
- Sohmer, B., Hudson, C., Hudson, J., Posner, G. D., Naik, V. Transesophageal echocardiography simulation is an effective tool in teaching psychomotor skills to novice echocardiographers. Can J Anaesth. 61 (3), 235-241 (2014).
- Sigounas, V. J., et al. Evaluation of simulation-based training model on vascular anastomotic skills for surgical residents. Simul Healthc. 7 (6), 334-338 (2012).
- Dawe, S. R., Windsor, J. A., Broeders, J. A., et al. A systematic review of surgical skills transfer after simulation-based training: laparoscopic cholecystectomy and endoscopy. Ann Surg. 259 (2), 236-248 (2014).
- Spadaro, S., Karbing, D. S., Fogagnolo, A., et al. Simulation Training for Residents Focused on Mechanical Ventilation. Simul Healthc. , (2017).
- Yee, J., et al. Mechanical Ventilation Boot Camp: A Simulation-Based Pilot Study. Crit Care Res Pract. 2016, (2016).
- Ryoo, E. N., Ha, E. H. The Importance of Debriefing in Simulation-Based Learning: Comparison Between Debriefing and No Debriefing. Comput Inform Nurs. 33 (12), 538-545 (2015).
- Shinnick, M. A., Woo, M., Horwich, T. B., Steadman, R. Debriefing: The Most Important Component in Simulation?. Clin Simul Nurs. 7 (3), e105-e111 (2011).
