Fifteen patients were included between March 2010 and November 2011. Six patients were included in phase I. Six patients were included in step 1 of phase IIa. Three patients were included in step 2 of phase IIa. A right or extended right hepatectomy was performed in all patients.Phase IIb is currently ongoing, and results are not described. Complete results of phases I and IIa have been previously published14.
Phase I:
In total, twelve HIFU ablations were successfully created in the six phase-I patients (Figure 5). One superficial HIFU ablation and one deep HIFU ablation were created in each of the 6 patients. Deep HIFU lesions were placed at a mean depth of 12 ± 2 (10–20) mm corresponding to a focal distance of 22 ± 2 (20–40) mm (Figure 3a). The resulting mean distance between Glisson's capsule and the HIFU ablation was, on average, 7 ± 4 (2–13) mm. Asepsis was not comprised in all patients during the preparation and utilization of the device. There was no lesion in neighboring tissues after HIFU ablation. There were no any substantial changes in respiratory and hemodynamic parameters. The duration of the HIFU procedure was, on average, 15 ± 7 (9–27) min. The ultrasound imaging probe integrated with the HIFU device allows visualizing, on average, 88% (95% CI: 67 to 100%) of the 15 predefined areas.
Phase IIa:
For the first three patients of step 1, the metallic mark had not been included in the HIFU lesions in one of six ablations. After reviewing the record of the procedure, it was established that a Glissonian pedicle was confused with the metallic marker (Figure 6). As required by the study design, three more patients were included, and all six additional HIFU lesions were correctly created around all six metallic markers. Since the primary objective of step 1 was achieved, the steering committee approved the continuation of the study.
The aim of step 2 was to achieve ablations distant from a metallic marker by 7.5 mm. Six ablations with a distance of 7.0 ± 2.3 (4.3–9.8) mm were achieved, demonstrating that it was possible to preserve an area from damage. The procedure was safe, asepsis was not compromised, and there was no lesion in the neighboring organs and no rupture of Glisson's capsule.
Common Secondary Objectives of Phases I and IIa:
All 30 HIFU ablations created in 15 patients were slightly cone-shaped. The average length of the HIFU ablations was 27.5 ± 6 mm. The average superior width of the HIFU ablations was 21 ± 3.9 mm. In ultrasound images, the average length of HIFU ablations was 28.9 ± 4.6 mm and the average superior width was 23.9 ± 3.8 mm. Figure 4b shows the rank correlation coefficient (r = 0.88; p < 0.001; 95% CI, 0.82 to 0.91) between macroscopic measurements and measurements performed using ultrasound images.
Figure 7 shows the capability of the imaging system to visualize metastases. Figure 7a and 7c show examples of two metastases imaged using the ultrasound imaging probe integrated with the HIFU device. Figure 7b and 7d show the corresponding metastases observed on gross pathology after surgery. The HIFU focal region was superimposed on the sonogram and displayed in the user interface, making it possible to place the location of the ablation with precision (Figure 7a).
As illustrated in Figure 8, the delimitation between treated and untreated liver is very sharp (about 200 µm). There was a halo of congestive tissues around all HIFU ablations. The microscopic examination confirmed homogeneous necrosis with all HIFU ablations. Since there were only 1 to 2 h between HIFU ablation and hepatectomy, it was not possible to observe evidence of apoptosis. However, pronounced alterations in hepatocytes were observed in all HIFU ablations. The microscopic analysis confirmed homogeneous ablations with all cases, notably around vessels (Figure 8).
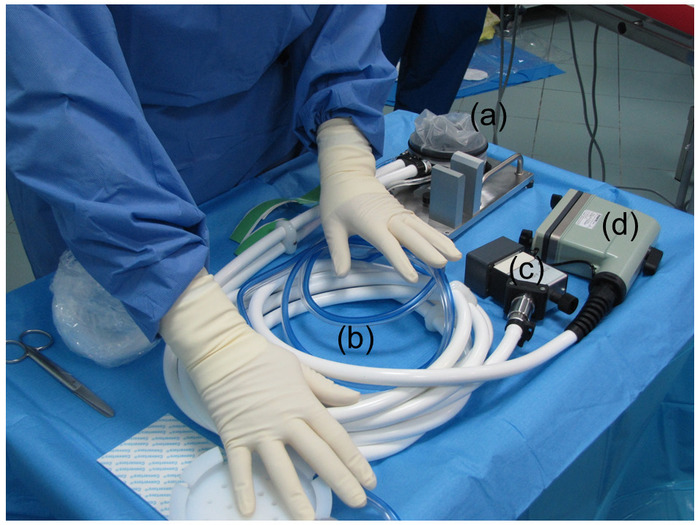
Figure 1: Preparation of the HIFU device. The HIFU device was prepared by covering the sterilized HIFU probe with a sterile envelope containing an ultrasound coupling liquid. (a) This panel shows the HIFU transducer covered with a sterile envelope. (b) This panel shows the tube for the cooling circuit. (c) This panel shows the connector for the electrical power. (d) This panel shows the connector for the ultrasound imaging probe. Please click here to view a larger version of this figure.
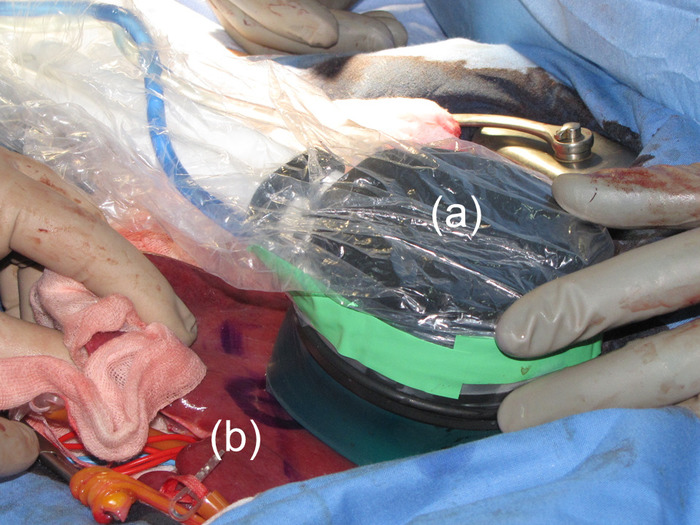
Figure 2: Use of the HIFU probe. The HIFU probe was held by hand and brought into contact with the liver surface. (a) This panel shows the HIFU probe. (b) The position of the HIFU probe at the time of ablation was marked on the liver. Please click here to view a larger version of this figure.
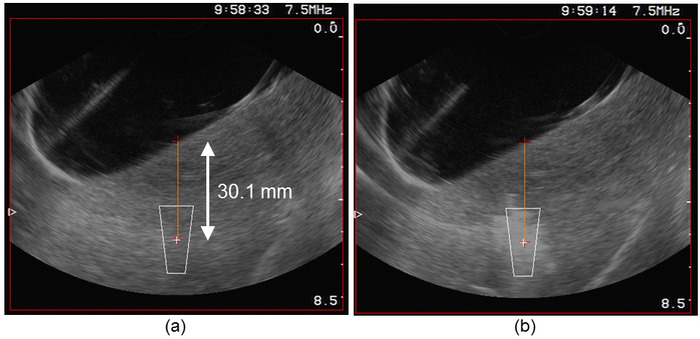
Figure 3: Targeting process. (a) The user interface displayed the position of the HIFU focal region superimposed on the sonogram, making it possible to place the location of the ablation in the tissues. (b) Immediately after the HIFU exposure, a cloud of ebullition appeared momentarily (for approximately 1 min) at the location of the lesion. Please click here to view a larger version of this figure.
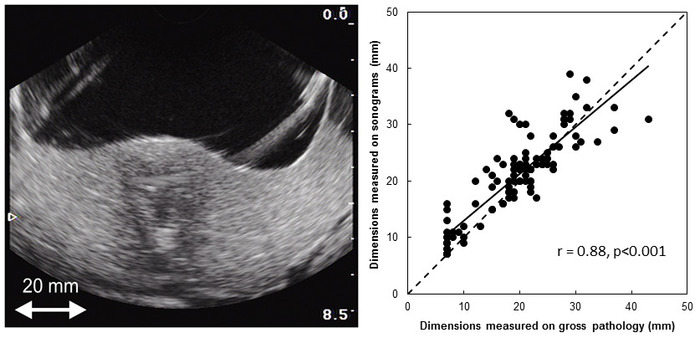
Figure 4: Monitoring. After boiling, the single lesion appeared on the sonogram as a hyperechoic zone at its center and a hypoechoic zone at its boundaries. Please click here to view a larger version of this figure.
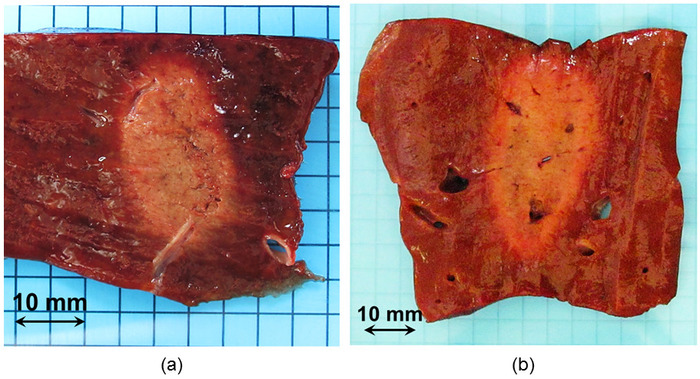
Figure 5: Macroscopic visualization of two HIFU ablations. HIFU ablations were clearly visible by gross pathology. (a) This panel shows a typical HIFU ablation. (b) This panel shows an example of a HIFU lesion created during step 1 of phase IIa. The aim was to target the metallic marker. The shape and homogeneity of the ablation were not altered by the presence of hepatic veins. Please click here to view a larger version of this figure.
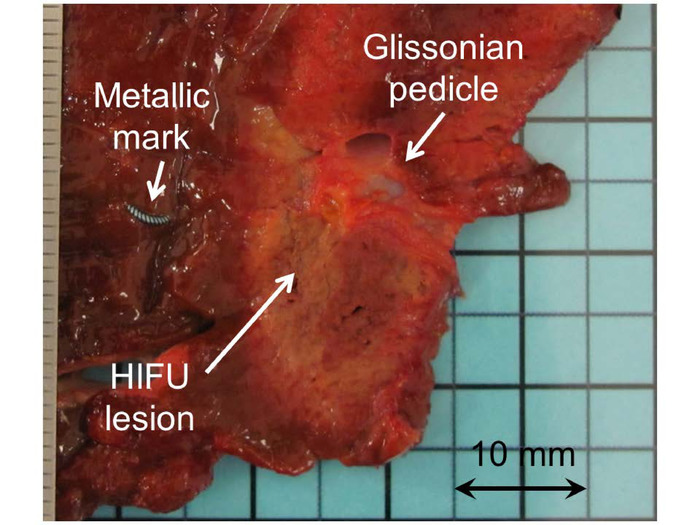
Figure 6: Macroscopic visualization of a HIFU ablation created in phase IIa. In one case, the metallic marker had not been included in the HIFU. After reviewing the record of the procedure, it was established that a Glissonian pedicle was confused with the metallic marker. Please click here to view a larger version of this figure.
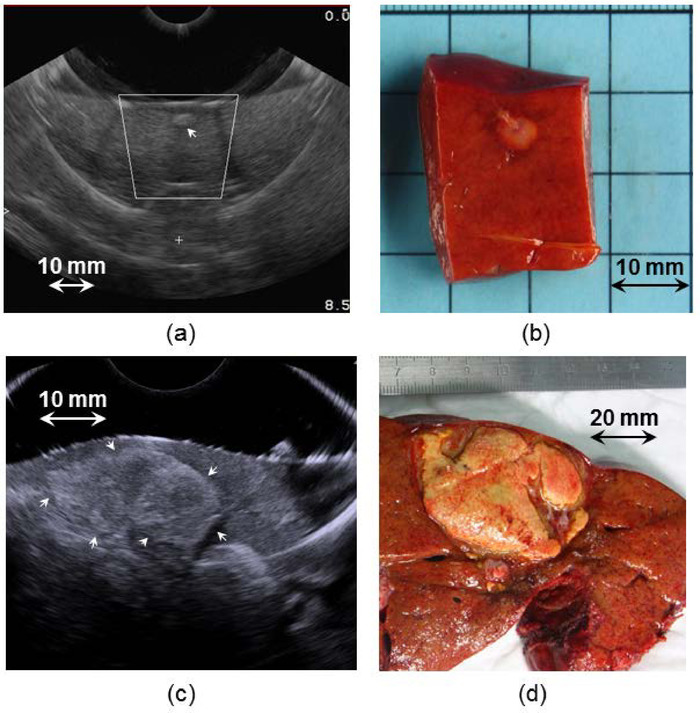
Figure 7: Visualization of metastases using the integrated ultrasound imaging probe. Panels (a) and (c) show examples of two metastases imaged using the ultrasound imaging probe integrated with the HIFU device. Panels (b) and (d) show the corresponding metastases observed by gross pathology after surgery. (a) The user interface displayed the position of the HIFU focal region superimposed on the sonogram, making it possible to place the location of the ablation in the tissues and to visualize if the metastasis will be treated with safety margins. Please click here to view a larger version of this figure.
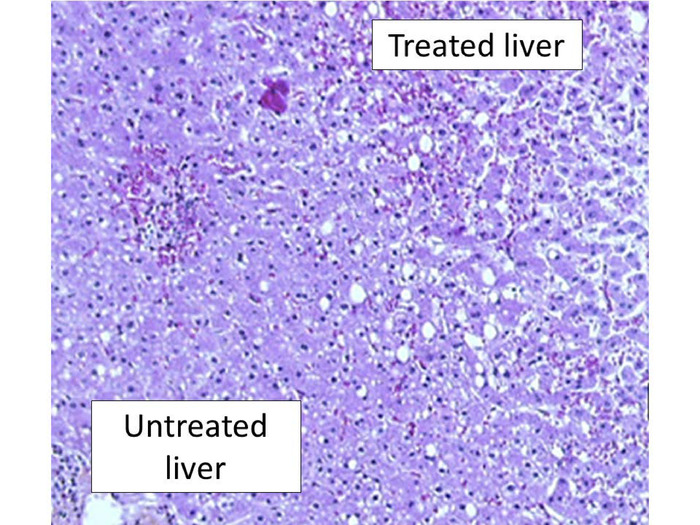
Figure 8: Histopathological examination after HIFU ablation. This panel shows a representative liver examination using H&E staining. There was a sharp demarcation between treated and untreated liver with pronounced alterations in hepatocytes. Here, the magnification is 200x. Please click here to view a larger version of this figure.
