Using a thoracic ultrasound, we found no pleural effusions on day 1 in all groups. However, on day 3, the pleural effusion appeared in the 6.25 and 12.5 mg/kg∙mL groups. The effusion was mainly in the right costal phrenic angle, while the pericardial effusion only presented in 12.5 mg/kg∙mL group. Furthermore, on day 7, both pleural effusion (Video 1) and pericardial effusion (Video 2) were detected in 6.25 mg/kg∙mL group (Figure 1). Pleural effusion increased slowly to the greatest extent on days 7-10 and then decreased gradually. On day 14, no pleural effusion was found anymore but with the sign of adhesion of pleura in all groups.10
At days 7 and 14, there were no signs of the pleural effusion in 3.125 and 6.25 mg/kg∙mL groups10. However, in the 12.5 mg/kg∙mL group, the chest CT scanning was abnormal with the blunt posterior costophrenic angle, which hinted at a small amount of pleural effusion (Figure 2a,b). No signs of the fluid level were observed, which was explained due to an insufficient amount of water.
Upon dissection of rats, we observed amber or colorless effusions in the 6.25 mg/kg∙mL and 12.5 mg/kg∙mL groups on days 3 and 7. The volumes of pleural effusion vary from 1-1.8 mL in each pleural cavity in the 6.25 mg/kg∙mL and 12.5 mg/kg∙mL groups. In the group of 3.125 mg/kg∙mL, no fluid in the pleural cavities appeared in the full experimental process.
With the TEM, the NPSi nanoparticles presented individually and clusters formed in the drained pleural fluid. The average diameter (Ø: 20 ± 5 nm) and the morphology in the pleural fluid were consistent with the NPSi in the prepared suspension. The nanoparticles were mostly spherical and well dispersed, and the average size of an individual nanoparticle was ~20 ± 5 nm (Figure 3a, b).
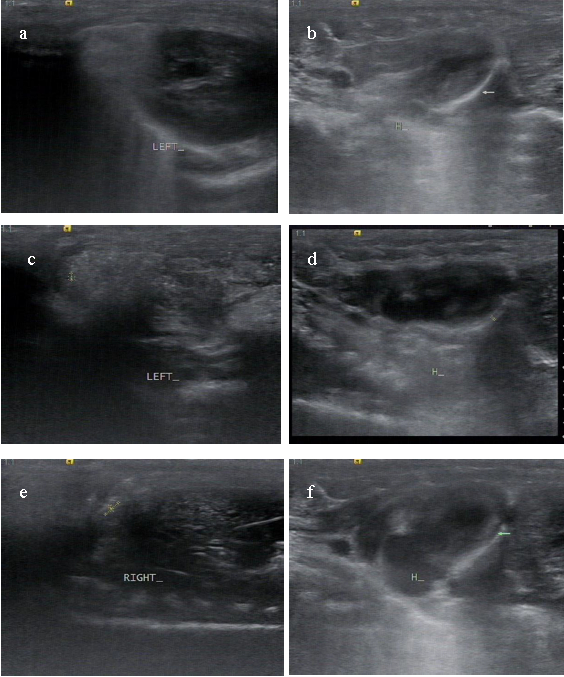
Figure 1: Representative images of pleural effusion by sonographic findings on day 7. (a, b) Sonographic images from a rat in the 3.125 mg/kg∙mL group with no fluid in pleural and pericardial cavities. (c, d) Sonographic images from a rat in the 6.25 mg/kg∙mL group with apparent pleural effusion and pericardial effusion. (e, f) Sonographic images from a rat in the 12.5 mg/kg∙mL group with much more fluid in pleural and pericardial cavities. Please click here to view a larger version of this figure.
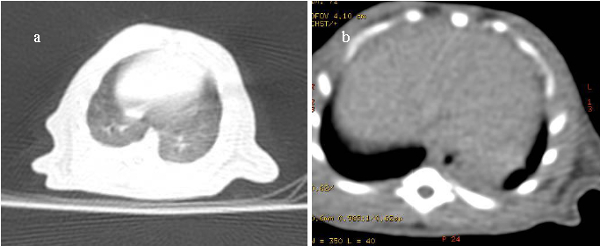
Figure 2. Representative images of thoracic CT images in rats. CT image from a rat in the 3.125 mg/kg∙mL group with no pleural effusion (a) and CT image from a rat in the 12.5 mg/kg∙mL group with a negative finding of free fluid but the blunt posterior costophrenic angle in the pleural cavity (b). Please click here to view a larger version of this figure.
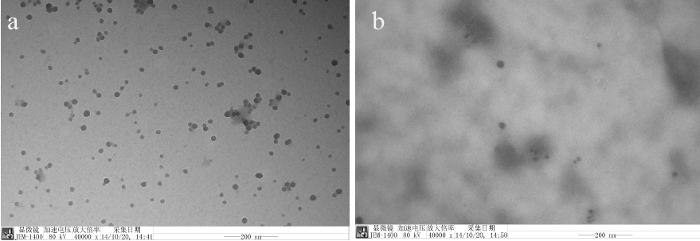
Figure 3. Silica nanoparticles in polyacrylate/nanosilica suspension and the pleural effusion of a rat. (a) Silica nanoparticles in polyacrylate/silica nanocomposite. (b) Silica nanoparticles in a rat's pleural effusion with clusters or individual form. Scale bar: 200 nm. Please click here to view a larger version of this figure.

Video 1. The pleural effusion in a rat in the 6.25 mg/kg∙mL group. Please click here to view this video. (Right-click to download.)

Video 2. The pericardial effusion in the rat in the 6.25 mg/kg∙mL group. Please click here to view this video. (Right-click to download.)
