The following procedure was conducted according to the Guidelines of the Use of Experimental Animals of the European Community. The experiments were also approved by the Animal Care Committee at the Ben-Gurion University of the Negev.
1. Animal selection and preparation
- Select 65 male Sprague-Dawley rats weighing 300 to 350 g with no overt pathology for this procedure. The smaller size poses technical difficulties for the MCAO procedure.
- Assign 3 rats per cage and let them adapt for least 3 days.
2. MCAO procedure
- Select 25 rats for MCAO allowing for 10—20% mortality associated with the procedure11.
- Perform MCAO using a standard technique, as previously described in detail12.
3. Laser-induced brain injury experimental procedure
- Assign 20 rats to a group marked as laser group and 20 rats to another control group (sham-operated).
- Subject the laser group rats to laser irradiation at 50J X 10 points in the following manner:
- Anesthetize rat with a mixture of 2% isoflurane in oxygen allowing for the spontaneous ventilation. Check for sufficient anesthetic depth by pinching the tail with forceps to see the absence of the withdrawal reflex.
- Maintain the core body temperature of the rat at 37 ˚C throughout the experimental procedure using a rectal temperature regulated heating pad.
- Remove local hair with a shaver and disinfect with 70% alcohol and 0.5% chlorhexidine gluconate. Repeat the disinfection step two more times.
NOTE: The size of the surgical incision should be approximately 3 cm. Remove hair at least 2 cm around the incision area. - Place the rat on a stereotaxic head holder in a prone position and make a 3 cm incision to reflect the scalp laterally and to expose the area between Bregma and Lambda.
- Maintain anesthesia through the nose cone.
- Use Neodymium-YAG (Nd-YAG) laser (peak wavelength 1064 nm) to administer 50J X 10 points, with 1 s pulse duration, to the exposed area of the skull above the right hemisphere.
- Ensure that the laser generating part of the apparatus is at a 2 mm distance from the exposed area to produce a laser beam. 50J X 10 points was selected after careful evaluation of different energy/surface combinations. This combination is efficient and does not cause bone destruction of the skull after administration for less than a second10.
NOTE: 2 mm is the distance between the terminal of the laser beam (from the optical cable it is passed through) and the skull bone. In case a focusing lens is used, the distance should be calculated taking into account the angle of inclination of the lens to focus the beam in the desired area of damage. Ensure proper safety when using a laser device including appropriate training and eye protection. - Remove the rat from the device and close the scalp with 3-0 silk surgical sutures.
- Discontinue anesthesia and return the rat to its cage for recovery. Administer 0.1 mL of 0.25% bupivacaine locally to reduce the postoperative pain immediately after surgery.
NOTE: The entire procedure should last less than 5 min if performed correctly.
- Observe the rat for any signs of distress during post- anesthesia recovery. Prior to emergence from anesthesia, give 0.01mg/kg intramuscular buprenorphine for postoperative analgesia and continue with repeated doses every 12 h for at least 48 h.
- Subject control rats to the same conditions without subjecting them to the laser.
4. Neurological severity score (NSS)
- Evaluate the neurological severity score 24 h after the laser-induced brain injury using a 43-point score13. Test the animals for neurological deficits, behavior disturbances, beam-balancing task, and reflexes, assigning higher scores for more severe disabilities, as previously detailed13.
5. Post-injury manipulations
- After NSS evaluation, euthanize the rats by exposing them to 20% oxygen and 80% CO2 (via inspiration) and transcardially perfuse the rat with heparinized phosphate-buffered saline (PBS, 0.9% NaCl).
NOTE: Ensure that CO2 is delivered at a predetermined rate in accordance with the Institutional Animal Care and Use Committee guidelines. This step may also be performed under 5% isoflurane anesthesia. - Harvest brains and prepare for further examination as described in an earlier protocol11.
- Evaluate for subarachnoid hemorrhage (SAH) through visual examination of the whole brain after its isolation from the skull. If necessary, a microscope or magnifying glasses may be used for this purpose.
6. Evaluation of the brain injury
- Determining the brain infarct volume and brain edema by TTC staining
NOTE: 2,3,5-Triphenyltetrazolium chloride (TTC) staining is a convenient procedure for brain infarct detection11.- Section the harvested brains into 6 coronal slices, each 2 mm thickness.
- Incubate the set of slices from each brain for 30 min at 37 °C in 0.05% TTC.
- Following staining, scan the slices with an optical scanner with a resolution of 1600 X 1600 dpi.
- The unstained areas of the fixed brain slices are defined as infarcted12.
- Using an image processing software (e.g., freeware Image J) measure the unstained infarcted area, ipsi- and contralateral hemispheres for each of the 6 coronal slices.
- Calculate the infarcted volume as a percentage of the total brain:

- Calculate brain edema using Kaplan method:

- Determining the extent of blood brain barrier (BBB) breakage
NOTE: Assess BBB breakage 24 h after the laser-induced brain injury as follows:- Administer 2% Evans Blue mixed with 4 mL/kg saline solution intravenously to rats via the cannulated tail vein and allow the solution to circulate for 1 h.
- Euthanize rats by exposing them to 20% oxygen and 80% CO2 (via inspiration) 24 h after the last NSS, as previously described13.
- Harvest the intravascularly localized dye as follows:
- Open the chests of the rats with surgical pincettes and surgical scissors.
- Perfuse the animals with cooled 0.9% saline via the left ventricle using 110 mmHg until obtaining a colorless perfusion liquid from the right atrium.
- Harvest the brains and slice them rostrocaudally into 2 mm slices.
- Separate the left brain slices from the right portions to evaluate injured and non-injured hemispheres separately.
- Weigh, homogenize using mortar and pestle, and then incubate the brain tissues in 50% trichloroacetic acid for 24 h.
- Centrifuge the homogenized brain slices at 10,000 × g for 20 min.
- Mix 1 mL of the supernatant from the centrifuged brain with 1.5 mL of 96% ethanol at 1:3 and assess blood-brain barrier breakage using a fluorescence detector at 620 nm excitation wavelength (10 nm bandwidth) and 680 nm emission wavelength (10 nm bandwidth).
NOTE: Both groups of rats undergo the same protocol for determining BBB breakdown.
No deaths or SAH were registered in either the control or experimental groups (Table 1). The MCAO group had a 20% rate of both mortality and SAH.
The relative body temperature changes in the rats of both groups were also similar, despite a difference in the variability of both groups (Table 1).
There was a significantly worse NSS in both the laser (16 ± 1.1) and MCAO (20 ± 1.5) models, compared to the sham-operated control group (1 ± 0.3; Table 1; p<0.01).
The laser-induced brain injury also caused a significant increase in infarct volume at the target hemisphere, compared to the sham-operated control group (2.4% ± 0.3 vs 0.5% ± 0.1; Table 2 and Figure 1A; p<0.01), per the Mann-Whitney U test. However, the infarct volume of the laser model was smaller in comparison to the MCAO technique (2.4% ± 0.3 vs 9.9% ± 2.9).
Brain edema determined 24 h after brain injury are shown in Figure 1B and Table 2. There was no difference in brain edema between the laser-induced brain injury model and the sham-operated control group (3.4% ± 0.6 vs 0.7% ± 1.2). There was a significant difference in brain edema between the laser model and the MCAO technique (3.4 ± 0.6 vs 7 ± 2.6†). Data are presented as mean ± SEM.
Compared to the sham-operated control group, the laser-induced brain injury and MCAO technique both caused a significant increase in BBB breakage at the non-injured hemisphere (563 ng/g ± 66 and 1176 ng/g ± 168, respectively, vs 141 ng/g ± 14; Figure 2A and Table 2; p<0.01) and target hemisphere (2204 ng/g ± 280 and 2764 ng/g ± 256, respectively, vs 134 ng/g ± 11; Figure 2B and Table 2; p<0.01).
Histological examination of rats’ brains are shown in Figure 3.
| NSS | Temperature, °C | SAH, % | Mortality, % | |||
| Groups | mean ± SEM | variability, % | mean ± SEM | variability, % | ||
| Sham-operated control | 1 ± 0.3 | 97 | 37.2 ± 0.1 | 59 | 0 | 0 |
| Laser 50J x10 | 16 ± 1.1* | 30 | 37.4 ± 0.1 | 84 | 0 | 0 |
| p-MCAO | 20 ± 1.5* | 37 | 38.3 ± 0.1* | 129 | 20* | 20* |
Table 1: Assessment of NSS, body temperature, subarachnoid hemorrhage, and mortality. * = p < 0.01
| BBB | Infarcted Volume | Brain Edema | ||||
| Groups | mean ± SEM | variability, % | mean ± SEM | variability, % | mean ± SEM | variability, % |
| Sham-operated control | 134 ± 11 | 25 | 0.5 ± 0.1 | 77 | 0.7 ± 1.2 | 573 |
| Laser 50J x10 | 2204 ± 280* | 40 | 2.4 ± 0.3* | 34 | 3.4 ± 0.6 | 58 |
| p-MCAO | 2764 ± 256* | 29 | 9.9 ± 2.9* | 92 | 7 ± 2.6* | 115 |
Table 2: Assessment of BBB breakdown, infarct zone, and brain edema. * = p < 0.01
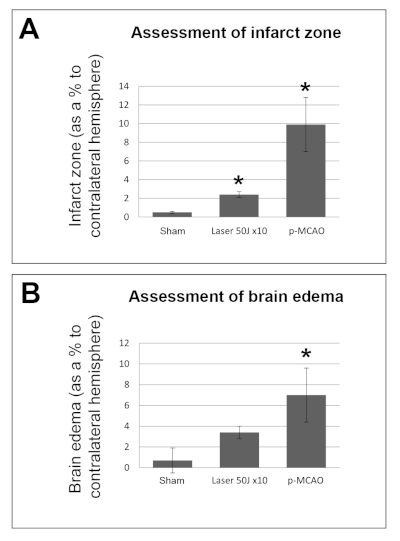
Figure 1: Assessment of brain injury in the laser model 24 h after the injury compared to the MCAO model and sham-operated control. (A) Assessment of infarct volume. There was an increase in infarct volume in the laser model compared to the sham-operated control (*p<0.01). However, the infarct volume in the laser model was smaller compared to the MCAO model (*p<0.01). (B) Assessment of total brain edema. There was an increase in brain edema in the MCAO model compared to either the laser model or sham-operated control. There was no difference in brain edema between the laser model and sham-operated control. The data are measured as % to the contralateral hemisphere and expressed as mean ± SEM. Please click here to view a larger version of this figure.
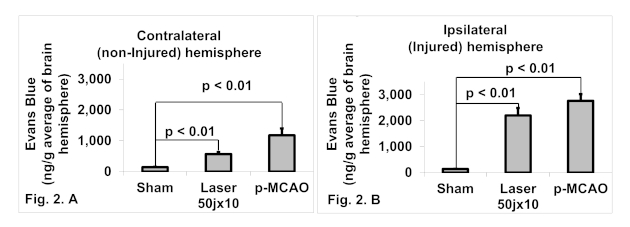
Figure 2: The extent of BBB breakdown compared to sham controls. (A) Contralateral (non-injured) hemisphere. Both the laser and MCAO models, led to a significant increase in BBB breakage at the non-injured hemisphere compared to the sham-operated control group (*p<0.01). (B) Ipsilateral (injured) hemisphere. There was a difference in ipsilateral BBB breakdown in the laser and MCAO models compared to the sham-operated control (*p<0.01). Please click here to view a larger version of this figure.
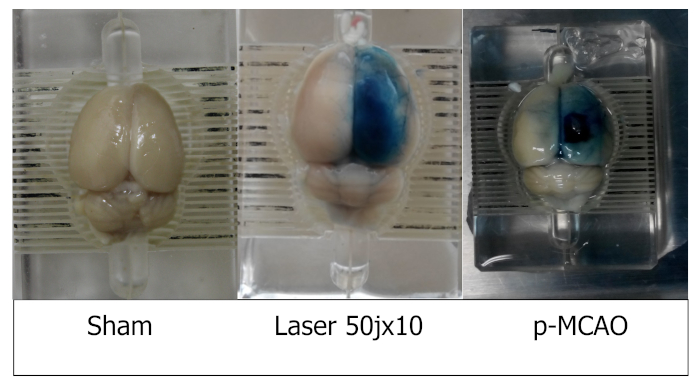
Figure 3: Histological examination of rats’ brains from sham, laser and MCAO groups. Please click here to view a larger version of this figure.
