The Washington University Institutional Animal Care and Use Committee (IACUC) approved all mouse infections and procedures as part of protocol number 20170081, which expired 06/09/2020, and 20-0031, which expires 03/18/2023. Overall care of the animals was consistent with The Guide for the Care and Use of Laboratory Animals from the National Research Council and the USDA Animal Care Resource Guide. Euthanasia procedures are consistent with the AVMA Guidelines for the Euthanasia of Animals: 2020 Edition.
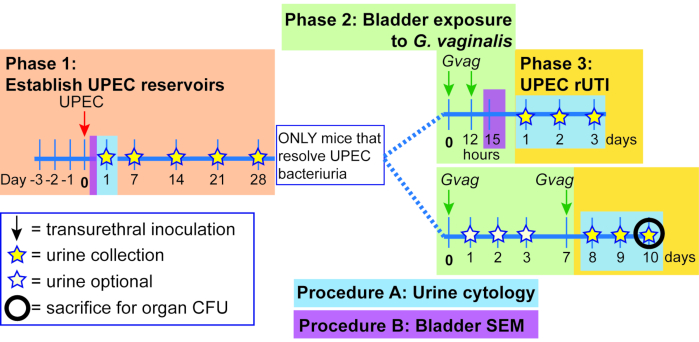
Figure 1. Schematic of Mouse Model. The timeline is highlighted to reflect the phases or procedures of the model outlined in the protocol. Phase 1 (orange): Establishing intracellular UPEC reservoirs. Mice are transurethrally inoculated with UPEC and urine samples are collected and monitored for clearance of bacteriuria. Only mice clearing bacteriuria proceed to the subsequent phases. Phase 2 (green): Bladder exposure to G. vaginalis. Mice are inoculated transurethrally with G. vaginalis two times. The duration of time between the two sequential exposures is either 12 h (top panel) or 1 week (wk; bottom panel), depending on the desired downstream analysis. Phase 3 (yellow): UPEC rUTI. Urine is collected daily following G. vaginalis exposure and monitored for UPEC bacteriuria. Additionally, bladders and kidneys can be collected at the experimental endpoint to measure UPEC tissue titers. In the 1 wk exposure model, G. vaginalis-induced emergence of UPEC from intracellular reservoirs and subsequent clearance from the urinary tract are also reflected in a decrease in UPEC bladder tissue titers (compared to PBS-exposed mice, see Figure 3D). This decrease in bladder titers was not evident in the 12 h exposure model, presumably because more time is required for sufficient reservoir emergence and clearance to occur to significantly reduce tissue titers. Procedure A: Urine cytology is typically performed 1 dpi (or even earlier) during Phase 1 to examine acute UPEC infection and during Phase 3 to assess the urine PMN content, which correlates with UPEC emergence. Urine samples collected at other timepoints can be similarly analyzed. Procedure B: Bladder scanning electron microscopy (SEM) to examine urothelial exfoliation is typically performed in the 12 h model at 3 h after the second G. vaginalis exposure (15 h after administering the first exposure at time 0). Other timepoints can also be assessed, such as 6-24 h after UPEC inoculation as shown in Phase 1. Please click here to view a larger version of this figure.
1. Establish UPEC quiescent intracellular reservoirs in mice
- Prepare urinary catheters (refer to 44,45,46,47 for videos of this step).
- Thread 30 Gauge needles with a length of PE10 tubing extending from the needle base to several mm beyond the needle tip. Take care to not puncture the tubing with the needle tip. Alternatively, use pediatric intravenous cannulas46.
- Place prepared catheters in a petri dish and sterilize with UV light for at least 30 min. Replace petri dish lid and secure for storage until needed.
- Prepare UPEC inoculum (Day -3 to 0)
- Day -3: Streak UTI89kanR from -80 °C freezer stock onto a Luria-Bertani (LB) agar plate. Incubate plate at 37 °C for 18-24 h.
NOTE: It is not necessary to add kanamycin to the inoculum growth media because the kanamycin resistance is stably integrated in UTI89kanR. - Day -2: Inoculate 20 mL of LB broth in a sterile 125 mL flask with a single colony of UTI89kanR. Do not use a smaller flask because this culture method is important to induce expression of the UPEC type 1 pilus that is necessary for bladder adhesion.
- Incubate statically (without shaking) at 37 °C for 18-24 h. Do not add antibiotics to the growth medium. Only use fresh colonies on LB plates (18-24 h old) to start liquid cultures.
- Day -1: Subculture UTI89kanR by removing 20 µL of culture (gently swirl the flask to resuspend settled bacteria) and adding to 20 mL of fresh LB broth in a sterile 125 mL flask. Incubate as in step 2, except for a firm 18 h duration. Do not add antibiotics to the growth medium.
- Day 0: Transfer entire culture into a 50 mL tube and spin at 3200 × g in a tabletop centrifuge for 10 min to pellet bacteria. Aspirate supernatant and resuspend the bacterial pellet in 10 mL of PBS.
- Add 100 µL of the concentrated bacterial suspension from step 4 to 900 μL of PBS in a cuvette and determine the optical density at 600 nm (OD600) using a spectrophotometer that has been blanked with PBS. Multiply the spectrophotometer value by 10 (to account for the dilution) to determine the OD600 of the suspension (ODsuspension).
- To achieve the desired inoculum concentration of 1 x 107 CFU in 50 µL, dilute (or concentrate) the UTI89kanR suspension using the following equation, in which the desired ODinoculum is 0.35 (value may vary for other UPEC strains) and Y is the volume of inoculum required (100 µL per mouse to allow extra for eliminating bubbles and filling the catheters):
X mL x ODsuspension = Y mL x ODinoculum
For example, if the ODsuspension value is 4.7 and 5 mL of inoculum are required:
X mL × 4.7 = 5 × 0.35
X = (5 × 0.35) / 4.7
X = 0.372 mL
Therefore, add 372 μL of bacterial suspension to make 5 mL (final volume) - Use a multi-channel pipette to make 1:10 serial dilutions of the inoculum out to 10-6 in sterile PBS in a 96-well plate. Spot five 10 µL replicates of all 6 dilutions onto an LB and LB+kan plate, allow the spots to dry, and incubate at 37 °C overnight. The LB plate without antibiotics is used to ensure the inoculum was not contaminated by another organism (which would appear as an additional colony morphology not present on the kan antibiotic selection plate). Both plate types should yield the same result.
NOTE: Plates should be allowed to dry on the benchtop for a day prior to use so that they will absorb the plated liquid without spots coalescing. - Count the total number of colonies in all spots of the dilution with distinguishable colonies and use the value to calculate the actual inoculum dose used in each experiment. Do not simply rely on the OD600 values.
- Day -3: Streak UTI89kanR from -80 °C freezer stock onto a Luria-Bertani (LB) agar plate. Incubate plate at 37 °C for 18-24 h.
- Inoculate UTI89kanR into the bladders of anaesthetized female mice (Day 0)
NOTE: Video recordings of this procedure have been published previously44,46. Refer to these papers for a more thorough description. See section 5 of this protocol for more detail on mouse catheterization.- Anesthetize mice with isoflurane inhalation according to IACUC-approved methods.
- While awaiting mice to become anesthetized, fill tuberculin syringe with UTI89kanR inoculum and then affix a prepared catheter. Depress the plunger to void air from the catheter, then dab the catheter into sterile surgical lubricant.
- Position the mouse on its back and confirm anesthetization by firmly squeezing the mouse footpad and observing the absence of a reflex or response. Locate the bladder (feels like a pea in the lower abdomen) between the forefingers of each hand. Express urine by moving fingers toward each other to apply a gentle squeezing pressure to the bladder.
- Insert the catheter through the mouse urethra into the bladder and slowly deliver 50 µL of inoculum.
- Wait a few seconds and then gently remove the catheter by pulling straight out. Return the mouse to its cage and monitor until it recovers from anesthesia.
- Repeat steps 1.3.1 – 1.3.5 with additional mice, changing the catheter between each cage (5 mice). If desired, the same procedure can be used to inoculate a control group of mice with PBS, for example to show another strain of G. vaginalis elicits rUTI (over the spontaneous/background level).
2. Monitoring clearance of UPEC bacteriuria (Days 1 to 28)
NOTE: Video of the urine collection procedure has been published previously44.
- Collect urine (minimum 10 µL) from all mice by bladder palpation as described44 at 1 d post infection and weekly for 4 wk (7, 14, 21 and 28 d post infection). Urine should be cultured within a few hours of collection in order to monitor UPEC infection. Store urine at 4 °C until plated. Urine can also be used for cytology (see Section 4). Occasionally if the bladder is very inflamed, 10 µL of urine cannot be obtained; in this case PBS can be added up to 10 µL, but the urine bacterial titer and cytology scores must be adjusted accordingly (e.g., if only 5 µL urine is collected and 5 µL PBS is added, multiply titers and scores by 2).
- With a multi-channel pipette, make 1:10 serial dilutions out to 10-6 in sterile PBS in a 96-well plate. Use a P10 multi-channel pipette to spot 10 μL of all 6 dilutions from column 1 in a vertical orientation on the left edge of an LB plate containing the relevant antibiotic selection marker. Discard tips.
- Repeat the plating with the remaining samples (column 2, then column 3, etc.). A single plate can accommodate 5 samples side-by-side. This produces a plate with a 5 × 6 spot matrix, with increasing dilutions from top to bottom and increasing sample numbers from left to right (Figure 2A).
- Allow the spots to dry on the benchtop, then incubate at 37 °C overnight. The next day, count the number of colonies in the least diluted spot in which the colonies are distinct (Figure 2B) and use this number to calculate CFU/mL:
# of colonies in single urine spot × dilution factor × 100 = CFU/mL urine - Plot UTI89kanR urine titers using graphing software (Figure 2C). Identify mice that have no detectable UTI89kanR in urine at 28 d (~65-80% of C57BL/6 mice). These mice harbor quiescent intracellular reservoirs and are used in the subsequent experimental phase to examine induction of recurrent UTI. Those with bacteria in urine at 28 d are not included in the subsequent steps.
3. Bladder exposures to G. vaginalis
- Assign mice to exposure groups (Day 29). The primary goal of this step is to avoid having all of the mice with more prolonged bacteriuria together in the same exposure group, since it is unknown whether this affects the likelihood of rUTI.
- Using the urine CFU data (Figure 2D), categorize the mice based on the time point at which UTI89kanR bacteriuria was no longer detectable (Figure 2E).
- Randomize the mice from each category into either the G. vaginalis or PBS inoculation groups; e.g., half the mice who cleared before day 7 get G. vaginalis and half will get PBS; half the mice who cleared between days 8 and 14 will get G. vaginalis and half will get PBS, etc. (as in Figure 2E).
- Prepare G. vaginalis inoculum (all steps performed in an anaerobic chamber)
NOTE: Ideal culture incubation times vary among different strains of G. vaginalis, with some strains entering the stationary phase and even beginning to die more quickly than others. This is particularly important given that killed G. vaginalis (JCP8151B) was unable to trigger rUTI39. Thus, incubation times should be determined empirically for a given strain prior to performing experiments in mice. It is unknown whether other/all strains of G. vaginalis will trigger the same effects in this model.- Streak G. vaginalis strain from -80 °C freezer stock onto an NYCIII plate (without antibiotics). Incubate plate at 37 °C anaerobically for 24 h.
- In the anaerobic chamber, inoculate 5 mL of anaerobic NYCIII media with a 1 μL loopful of cells (a single colony is insufficient) from the NYCIII plate and incubate culture statically at 37 °C under anaerobic conditions for 18 h. Do not include antibiotics in the growth medium.
- Determine the OD600 of the culture using a spectrophotometer.
- Centrifuge a defined volume (X) of culture at 9600 × g for 1 min and aspirate the media. Calculate the volume (Y) of PBS to re-suspend the pellet to achieve the desired inoculum OD to achieve 108 CFU in 50 μL using the following equation:
X mL × ODculture = Y mL × ODinoculum solve for Y
Y = (X ml × ODculture) / ODinoculum
NOTE: The ODinoculum for JCP8151BSmR is 5 but this must be determined empirically for other G. vaginalis strains. For example, if spinning 3 mL of an JCP8151BSmR overnight liquid culture with ODculture = 2.0: Y= (3 mL × 2.0) / 5.0; therefore resuspend pellet in 1.2 mL PBS - Resuspend the bacterial pellet in PBS to the desired concentration. Serially dilute and plate the inoculum (as described in CFU plating protocol above) to determine the actual inoculum dose that has been used in each experiment. Do not simply rely on the OD values.
- Centrifuge a defined volume (X) of culture at 9600 × g for 1 min and aspirate the media. Calculate the volume (Y) of PBS to re-suspend the pellet to achieve the desired inoculum OD to achieve 108 CFU in 50 μL using the following equation:
- On Day 29-31 following UPEC inoculation, inoculate anesthetized mice with G. vaginalis or PBS as described in step 1.3 above. A PBS control group is essential, as the act of catheterizing the bladder could possibly induce damage and urothelial exfoliation that could elicit some degree of UPEC reservoir reemergence. PBS-inoculated mice therefore serve as the control to which G. vaginalis-inoculated mice are compared.
NOTE: The final UPEC bacteriuria determination at 28 d requires overnight incubation of the CFU plate. Therefore, the earliest this step can be performed is 29 days following the initial UPEC inoculation. If necessary, the exposure could be given as late as day 31. Researchers should be consistent between experiments. - Repeat the inoculum preparation to administer a second G. vaginalis (or PBS control) inoculation at the desired time point, such as 12 h or 1 wk after the first inoculation. A second exposure is necessary because a single inoculation with G. vaginalis does not result in significant UPEC emergence39.
4. Monitoring UPEC recurrent UTI
- Collect urine from mice at desired time points following each G. vaginalis inoculation (1, 2, and 3 d post-inoculation recommended).
- Serially dilute and plate urine on selective plates (e.g., LB+kanamycin) to determine UTI89kanR CFU/mL. If desired, urine dilutions can also be plated on selective plates (e.g., NYCIII + 1 mg/mL streptomycin) to determine G. vaginalis CFU/mL. However, G. vaginalis JCP8151BSmR was cleared from the urine of most mice by 12 h 39. Therefore, earlier timepoints would be necessary to detect G. vaginalis in most mice.
- At the experimental endpoint (e.g., 3 d after the second G. vaginalis inoculation), sacrifice the mice according to approved methods (e.g., cervical dislocation under isoflurane anesthesia or CO2 inhalation) and collect bladders and kidneys for CFU enumeration, as described previously 44,46.
5. Urine cytology
NOTE: This procedure can be performed at any timepoint at which visualization of the cells and/or bacteria present in urine is desired. As indicated in Figure 1, urine cytology is typically performed at 1 dpi (or even earlier) during Phase 1 to examine acute UPEC infection and during Phase 3 to assess the presence of polymorphonuclear (PMN) cells in urines that display UPEC emergence.
- Add 10 µL of urine to 90 µL of PBS in a cytofunnel cassette with attached filter and slide. (The simplest method is to use the remainder of the 1:10 dilutions from the 96-well plate used for urine culturing; these samples can be used up to 24 h after urine culturing if stored at 4 °C). Place cassettes in cyto-centrifuge and spin at 600-800 x g for 6 min with high acceleration.
- Remove slides and allow to dry overnight. The next day, stain with a hematology staining kit (e.g., Wright's, Giemsa, including fixative) according to the manufacturer's protocol.
- Analyze the slides by light microscopy for the presence of PMNs and epithelial cells. If desired, these can be scored using a qualitative scoring metric based on the abundance of each cell type present in each high-powered field of view (e.g., 0=none, 1=few, 2= moderate, 3=robust). Ensure that the individual analyzing the slides is blinded to the experimental groups to minimize potential bias.
6. Imaging bladders by scanning electron microscopy
NOTE: This procedure can be performed at any timepoint at which visualization of the urothelium is desired. As indicated in Figure 1 (purple boxes), UPEC-urothelial interactions are best visualized between 6 h and 24 h post UPEC inoculation during the reservoir formation phase, and urothelial exfoliation triggered by G. vaginalis is best visualized between 3 h and 12 h after the second G. vaginalis exposure.
- In situ bladder fixation
- Prepare fixative immediately before bladder harvest by adding glutaraldehyde (2.5% final) and paraformaldehyde (2% final) in 0.15 M sodium cacodylate buffer with 2 mM of CaCl2 at pH 7.4. Use paraformaldehyde and glutaraldehyde from newly opened glass ampules, as both fixatives oxidize over time in opened containers.
CAUTION: Glutaraldehyde is toxic, a respiratory irritant, and corrosive; paraformaldehyde is flammable, carcinogenic, an irritant and a reproductive toxin; sodium cacodylate is toxic and carcinogenic. - To make 50 mL of fixative solution, add 6.25 mL of 16% paraformaldehyde, 2 mL of 50% glutaraldehyde, and 16.75 mL of ultrapure water to 25 mL of a 0.3 M solution of sodium cacodylate at pH 7.4 with 4 mM CaCl2.
- Warm the prepared fixative to 37 °C prior to administering to bladders.
- Fill tuberculin slip-tip syringe with fixative and affix a catheter to the end, bevel facing opposite syringe markings. Snip off the excess tubing 1-2 mm from the end of the needle, taking care not to expose the needle tip. Flick the syringe to remove bubbles and push the plunger to void air and fill the catheter with fixative over a microcentrifuge tube to collect any fixative for proper disposal.
- Anesthetize and sacrifice the mouse using an approved method (e.g., cervical dislocation under anesthesia). Place the mouse on dissecting surface with the legs secured (with rubber bands or pins). Open the mouse pelvic area with forceps and a pair of surgical scissors to expose the bladder. Carefully push aside the adjacent fat but leave the bladder in place.
- Hold the syringe with the dominant hand with the needle pointing down and the needle bevel and syringe markings facing away from you. Dip the catheter tip into sterile lubricant.
- Position the catheter tip at the urethral opening, holding the syringe barrel away positioned at a 30-45° angle over the mouse body.
- Apply downward pressure using a very small clockwise motion with the tip and gently insert the catheter into the urethra. As the catheter tip enters the urethra, hinge the syringe toward the tail of the mouse while continuing to slide the catheter further into the urethra until the syringe barrel is parallel to the working surface. The entire catheter needle shaft (not including the base) should enter the mouse, positioning the catheter tip within the bladder lumen.
- Slowly deliver 50-80 µL of fixative, causing the bladder to inflate like a balloon. Keep the catheter in place and raise the syringe slightly, tilting the tip up.
- With the other hand, open a hemostat and slide one prong under the catheter needle at the intersection of the urethra. Partially close the hemostat until it just makes contact with the needle.
- Gently slide the catheter needle out of the bladder while simultaneously clamping down and locking the hemostat completely to prevent loss of the fixative.
- Grip the hemostat so that it is parallel to the working surface with the bladder resting on top. Lift up gently and carefully cut under the hemostat (opposite side of the bladder) to remove the bladder with the hemostat still attached.
- Place bladder and attached hemostat into a Falcon tube containing warmed fixative. Ensure that the bladder is fully submerged in the fluid and not pressed against the walls of the tube. Incubate at 4 °C for 24 h.
- Prepare fixative immediately before bladder harvest by adding glutaraldehyde (2.5% final) and paraformaldehyde (2% final) in 0.15 M sodium cacodylate buffer with 2 mM of CaCl2 at pH 7.4. Use paraformaldehyde and glutaraldehyde from newly opened glass ampules, as both fixatives oxidize over time in opened containers.
- Bladder processing and imaging with scanning electron microscopy (SEM)
- Sagittally bisect the bladder with a cleaned, double-sided razor blade, and make a second cut tangential to the hemostat to release the bladder. This results in 2 half-bladder "cups." If any remaining fat pads exist on the exterior of the bladder, gently remove them.
- Rinse the bladder halves three times (10 min each) in sodium cacodylate buffer (0.15 M, pH 7.4).
- Stain the tissue with 1% osmium tetroxide in 0.15 M cacodylate buffer for 1 h at room temperature. Osmium is sensitive to light; therefore, perform this step with the staining vessel wrapped in foil to maintain a dark environment.
CAUTION: Osmium tetroxide is toxic and corrosive to skin. Do this step in the fume hood with gloves. - Rinse the bladder halves three times (10 min each) in ultrapure water. During these steps, osmicated oil can sometime be seen on the surface of the water. Aspirate or wick this off to prevent contamination during the drying steps.
- Dehydrate tissues by submerging in a graded ethanol series (50, 70, 90, 100, and 100%) for 10 min each.
- Dry the fixed tissue using a critical-point dryer performing 12 CO2 exchanges at the slowest speed. Set all additional settings to slow, except for the venting step which is set to fast.
- Bisect each bladder half again with a clean double-sided razor to generate 4 total pieces to reduce curvature of the specimen for more efficient coating, for ease of imaging in the SEM, and to expose tissue that may have curled during drying.
- Adhere the bladder pieces to a conductive carbon adhesive tab on an aluminum stub and paint a small amount of silver adhesive around the bottom contact with a toothpick, taking care to prevent excess adhesive from wicking onto the inner surface of the bladder.
- Use a high vacuum sputter coater to sputter coat the sample stubs with 6 nm of iridium. If the samples continue to charge, ensure a conductive path is painted to the surface with silver paint and coat with an additional 4 nm of iridium.
- Image the samples with a scanning electron microscope. While conditions may vary depending on the microscope used, an accelerating voltage of 3 KeV with a beam current of 200 pA and a working distance of 12-13 mm worked well on a Zeiss Merlin FE-SEM when using the Everhart-Thornley (SE2) electron detector.
Following inoculation, UPEC titers are detectable in urine (Figure 2B). Failure to plate urine samples on selective media containing kanamycin will likely result in overgrowth of endogenous mouse microbiota contaminating the urine. The level of UPEC bacteriuria will likely be high on day 1 and may increase during the first week before decreasing at later timepoints (Figure 2C). Approximately 65-80% of mice will have no detectable UPEC in the urine by 28 dpi (Figure 2C, green circle). These mice can be used in the subsequent steps of the model. Mice that remain bacteriuric (Figure 2C, red ellipse) should be eliminated from the experiment.
Two sequential G. vaginalis exposures given 12 h (Figure 3A) or 1 wk apart (Figure 3B) result in the emergence of UPEC from intracellular reservoirs to cause recurrent bacteriuria. Both the level of UPEC bacteriuria (Mann-Whitney test) and the fraction of mice displaying UPEC rUTI (Fisher's exact test) are significantly higher in mice exposed to G. vaginalis compared to the PBS control group. Urine cytology analysis detects PMNs in urine from G. vaginalis-exposed mice that displayed UPEC emergence (Figure 3C). In the model with two exposures given 1 wk apart, UPEC titers in bladder tissue are lower in G. vaginalis-exposed mice compared to PBS (Figure 3D), presumably due to emergence of UPEC from reservoirs and subsequent clearance.
Visualization of in situ-fixed bladder tissue by SEM reveals large superficial umbrella urothelial cells lining the bladder surface in control mice exposed only to PBS (Figure 4A). Urothelial exfoliation is evidenced by a loss of superficial umbrella cells, revealing smaller underlying transitional epithelial cells in mice exposed to G. vaginalis (Figure 4B). Early after UPEC inoculation during the establishment of intracellular reservoirs, UPEC are visible on the urothelium and filamenting out of exfoliating cells (Figure 4C).
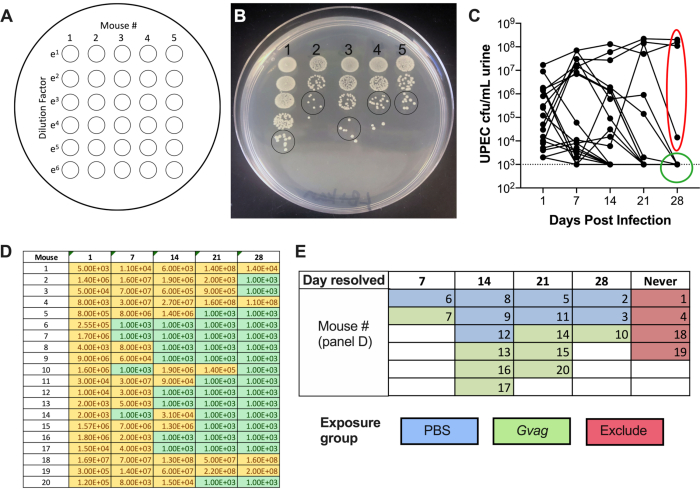
Figure 2. Monitoring UPEC titers in urine during Phase 1 (reservoir formation). (A) Schematic of colony-forming units (CFU) plating. (B) Representative image of UPEC titers in urine on LB+kanamycin. Black circles indicate urine sample spots that should be counted to calculate CFU/mL. (C) Time course of UPEC bacteriuria in C57BL/6 mice. Each line represents an individual mouse, tracing the UPEC urine titers over time. Dotted line indicates the limit of detection (1000 CFU/mL). Red ellipse indicates four mice (out of 20) that failed to resolve UPEC bacteriuria and would therefore not be used for the G. vaginalis-induced rUTI model. Conversely, green circle indicates mice that resolved UPEC bacteriuria and proceeded to subsequent phases. (D) Table of data used to generate graph in panel C. Yellow, detectable CFU; green, no CFU. (E) Randomization of mice into exposure groups based on the time point at which UPEC CFU were no longer detected in urine ("Day resolved"). The mouse numbers in the left column of panel D are the same mouse numbers given in panel E. Please click here to view a larger version of this figure.
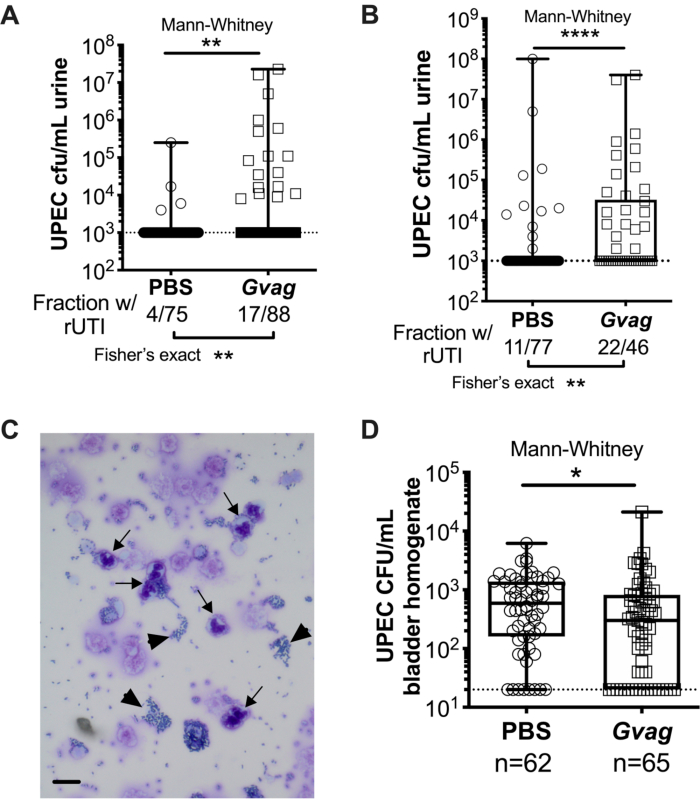
Figure 3. G. vaginalis triggers UPEC rUTI. UPEC titers in urine following two sequential urinary tract exposures to PBS (circles) or G. vaginalis (Gvag; squares) given 12 h (A) or 1 wk (B) apart. Each symbol represents an individual mouse. The highest CFU/mL UPEC detected from each mouse between 1-3 d following the second exposure are plotted. Mice with no detectable bacteriuria are plotted at the limit of detection (dotted line). (C) Urine cytology analysis showing UPEC (arrowheads) and polymorphonuclear (PMN) cells (arrows). Scale bar = 20 μm. (D) UPEC titers in bladder tissues collected 3 d following two sequential urinary tract exposures given 1 wk apart. Each symbol represents a different mouse and zeros are plotted at the limit of detection (dotted line). In A, B, and D, boxes are at the first and third quartile with the median marked and whiskers from min to max. Mann-Whitney U tests * P < 0.05; ** P < 0.01; **** P < 0.0001. Please click here to view a larger version of this figure.
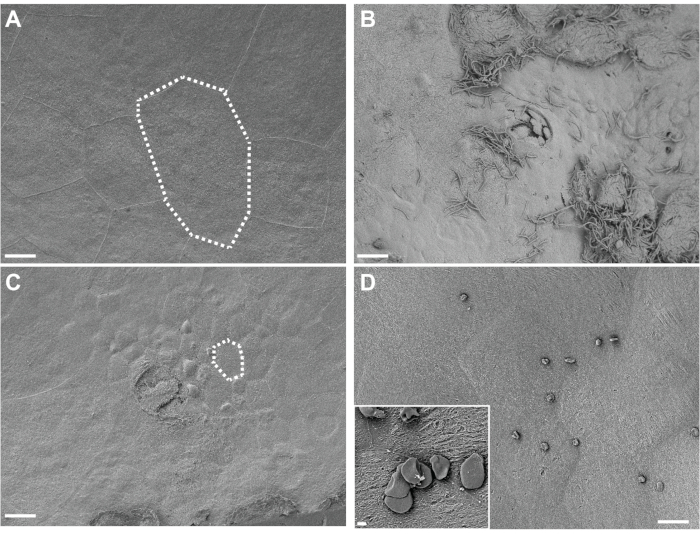
Figure 4. SEM analysis of bladders fixed in situ. Bladders were collected from mice 3 h after two exposures (12 h apart) to PBS (A) or G. vaginalis (C). Dotted lines illustrate a single urinary epithelial cell, which is smaller in G. vaginalis-exposed bladders because the large superficial cells have exfoliated away revealing the underlying transitional epithelium. (B) Bladder collected 6 h after initial inoculation with UPEC, during Phase 1 of the model, showing urothelial exfoliation and extracellular UPEC. (D) Example of insoluble fat droplets present on the bladder surface. Scale bars are 20 μm in the main images and 2 μm in the inset. Please click here to view a larger version of this figure.
