In order to measure pulmonary edema, the wet-to-dry weight ratio was calculated. The donor's native lobe, the transplanted lobe, and the recipient's native lobe were collected as described in the protocol and weighed immediately for wet weight, dried at 60 °C for 48 h, and then weighed again for the dry weight. An increased wet-to-dry weight ratio would be indicative of pulmonary edema. Our results indicate that the transplanted lobe did have a significant increase in wet-to-dry weight ratio compared to the donor's or recipient's native lobe (p=0.0050, n=6/group; Figure 11).
| Angio-catheter size for cuffs | |||
| Rat Body Weight (g) | PA | Br | PV |
| 180-200 | 20 G | 18 G | 16 G |
| 200-230 | 18 G | 16 G | 14 G |
| 230-250 | 18 G | 14 G | 14 G |
| 250-270 | 18 G | 14 G | 12 – 14 G |
| Over 270 | 16 G | 14 G | 12 G |
Table 1. Size Guide for Cuffs. The size of the pulmonary artery (PA), bronchus (Br), or pulmonary vein (PV) is related to body weight. Depending on the body weight and which type of cuff you are making, the recommended angio-catheter size is given.
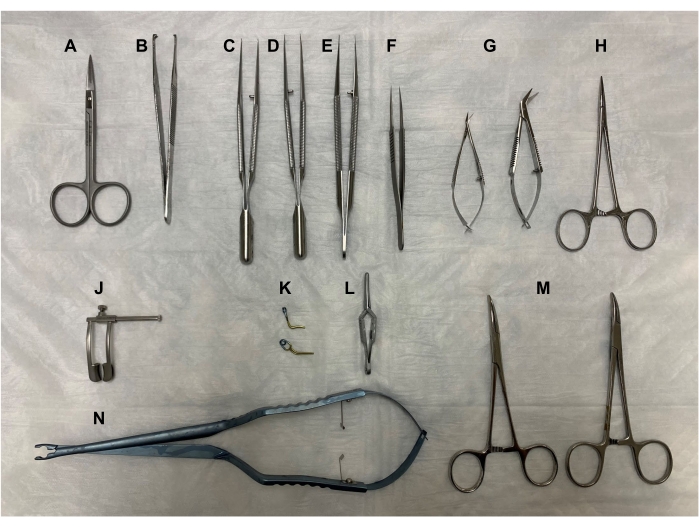
Figure 1. Surgical tools. (A) Fine scissors, (B) forceps, (C-E) microsurgical forceps, (F) Dumont #5 fine forceps, (G) Vannas-Tubingen spring scissors and Castroviejo micro dissecting scissors, (H) Halsted-mosquito hemostat, (J) retractor, (K) Yasargil clamps, (L) Dieffenbach bulldog clamp, (M) curved hemostats, and (N) Yasargil clamp applicator. All tools should be autoclaved at 121 °C for 30 min. Please click here to view a larger version of this figure.
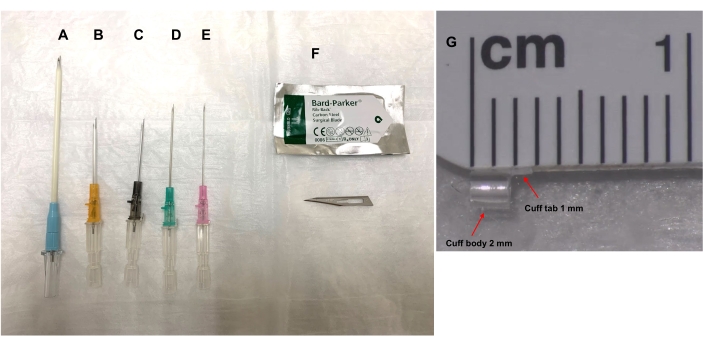
Figure 2. Cuff preparation with various sizes of angio-catheter and rib-back surgical blade #11. The size of the angio-catheter chosen for the cuff is determined by the cuff size guide (Table 1) that takes into account the rat's body weight and whether the cuff is for the pulmonary artery (PA), bronchus (Br), or pulmonary vein (PV). The angio-catheters (A) 20 G, (B) 18 G, (C) 16 G, (D) 14 G, or (E) 12 G are cut with a (F) rib-back surgical blade #11 as described in the protocol, and stored in saline until needed. (G) The cuff body length is 2 mm and a 1 mm X 1 mm tab (width x height) is left at the top of the cuff body for handling of the cuff body. Please click here to view a larger version of this figure.
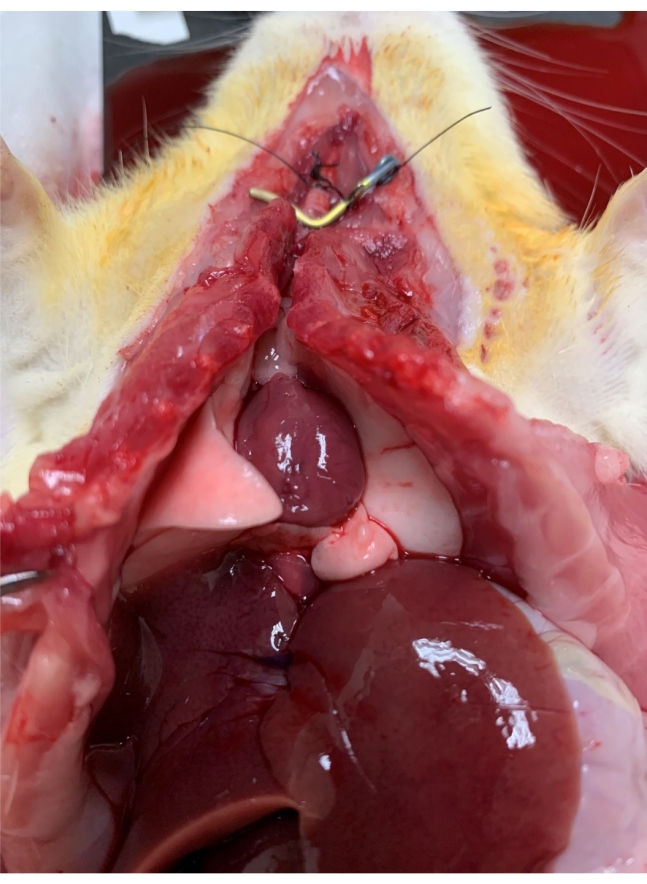
Figure 3. Warm ischemia. Lungs are flushed with the preservation solution through the pulmonary artery, inflated with twice the tidal volume of air, and then wrapped with an under pad and kept on the surgery warming board to keep the rat at normal body temperature for 1 h. Please click here to view a larger version of this figure.
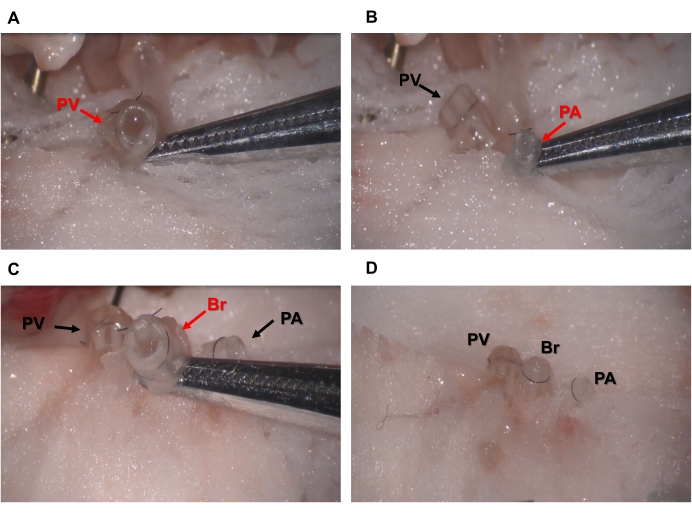
Figure 4. Cuffing of donor lung PV, PA, and Br. (A) Pulmonary vein, PV (B) pulmonary artery, PA, or (C) bronchus, Br, is inserted through a properly sized cuff, everted, secured with 8-0 nylon suture, and (D) then stored on sterile gauze dampened with ice-cold saline on a sterile Petri dish on ice. Please click here to view a larger version of this figure.
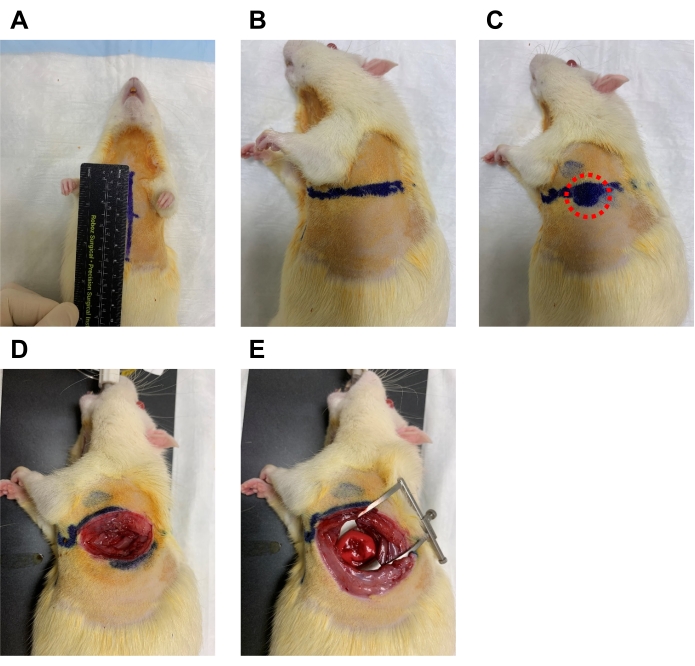
Figure 5. Measuring and dissecting at the 4th intercostal space. (A) The recipient rat is laid supine, and the chest is measured from the suprasternal notch to the xiphoid process and a line is drawn. (B) At the midpoint of this line, another line to the left side is drawn at half the length. (C) Along this line, the microsurgeon should feel for an area where the cardiac impulse is strongest to ensure the proper location of the 4th intercostal space (red circle). (D) The skin and muscle are then dissected with fine scissors. (E) The retractor is then used to open the space widely. Please click here to view a larger version of this figure.
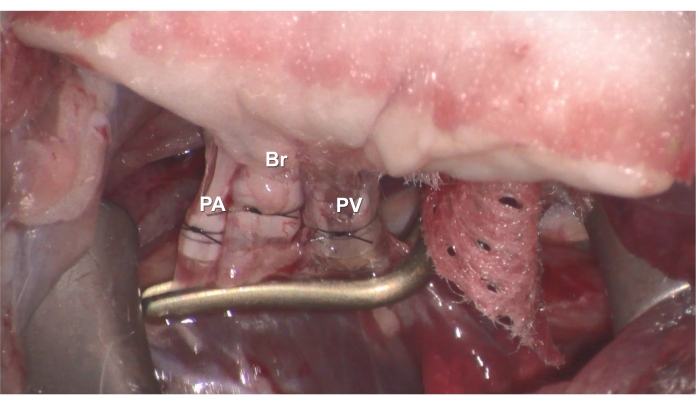
Figure 6. Anastomosis. The donor's cuffed (A) PV (B) Br, or (C) PA is inserted into the recipient's PV, Br, or PA, and then secured with 7-0 nylon suture. Please click here to view a larger version of this figure.
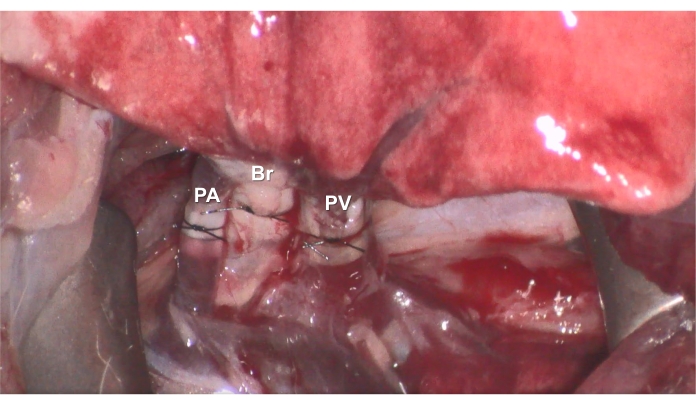
Figure 7. Reperfusion. After the anastomoses are complete, reperfusion can be started by removing the clamp, and the recipient rat is survived for 3 h under ventilation and anesthesia. Please click here to view a larger version of this figure.
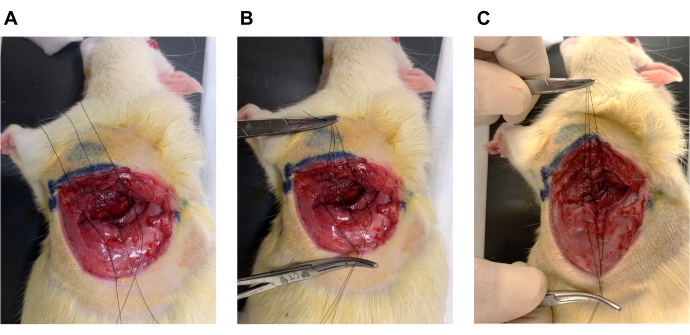
Figure 8. Wound closure. (A) Three 6-0 nylon sutures with simple double knots are placed around the ribs superior to the 4th rib and inferior to the 5th rib. (B) Use hemostats in both hands to gather the three sutures together and increase the PEEP to 6 cmH2O in the ventilation settings. (C) Tie together all three knots at the same time by pulling up and away to close the wound, decrease PEEP to 2 cmH2O immediately, and close skin with 6-0 nylon suture. Please click here to view a larger version of this figure.
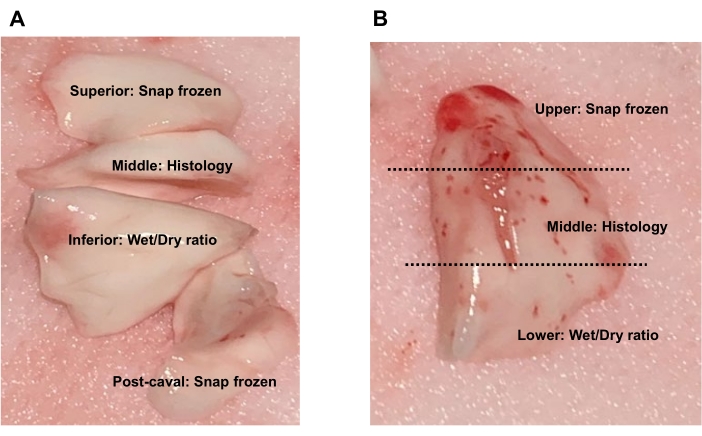
Figure 9. Lung tissue collection. (A) For the donor's or recipient's native lobes, the superior lobe and post-caval lobe can be snap frozen for protein or RNA expression analyses, the middle lobe can be preserved for histology, and the inferior lobe can be used for wet-to-dry weight ratio. (B) For the transplanted lobe, collect the upper region for snap frozen, middle region for histology, or lower region for wet-to-dry weight ratio. Please click here to view a larger version of this figure.
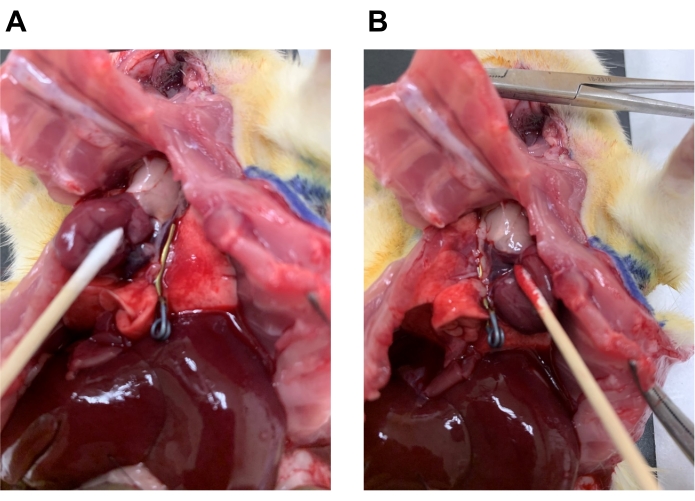
Figure 10. Application of the clamp for selective BAL fluid collection. To avoid a pooled sample, BAL fluid can be collected from either the right (native) or left (transplanted) lung. (A) The left lung hilar area can be clamped to collect BAL fluid from the right lobes. (B) The right lung hilar area can be clamped to collect BAL fluid from the left lobe. Please click here to view a larger version of this figure.
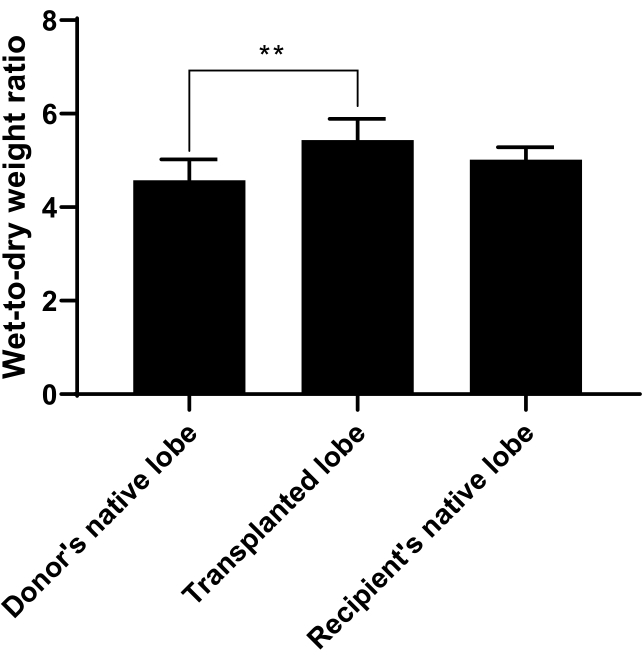
Figure 11. Wet-to-Dry Weight Ratio. Wet-to-dry weight ratio was calculated to measure pulmonary edema and can be used to indicate how well the transplant went. The donor's native lobe, the transplanted lobe, or recipient's native lobe was collected as described in the protocol and weighed immediately for wet weight, dried at 60 °C for 48 h, and then weighed again for the dry weight. A ratio of wet weight to dry weight was taken. The ratio for the transplanted lobe was significantly increased compared to the donor or recipient's native lobes. n=6 rats/group and bars represent mean ± SD. Statistical analysis was performed by using ANOVA with Tukey's post-hoc analysis. ** p<0.01. Please click here to view a larger version of this figure.
