From October 17, 2017 to April 6, 2018, we conducted the first quality assurance/quality control (QA/QC) audit of the 197 oscillometry tests3. Although all of the operators were trained prior to testing patient with a one hour seminar and on-site testing, 10 (5.08%) unacceptable and/or irreproducible measurements were identified. These measurements were excluded due to cough, tongue obstruction, and CoV greater than 15% following the initial suggested ERS guidelines52. Biologic quality control (BioQC) was not conducted regularly. The research personnel underwent additional oscillometry training and developed a standard operating protocol to ensure proper ERS guidelines and medical professionalism were in place. The importance of BioQC, a tool to validate testing equipment and procedures, was highlighted to the research personnel, who were reminded to perform regular BioQC tests.3 Improvements were found in subsequent QA/QC audits. Out of the total of 1930 oscillometry tests conducted from April 9, 2018 to June 30, 2019, only three (0.0016%) tests were invalid measurements; these had CoV greater than 15%. Between July 2, 2019 and March 12, 2020, there were 1779 oscillometry tests performed and nine (0.005%) were considered unacceptable, including measurements that had glottis closure, air leakage, and CoV greater than 15%. Refer to Table 1 for additional information.
Since the reinforcement of BioQC in April 2018, research personnel conducted BioQC regularly. At our center, four healthy non-smoking individuals conducted oscillometry daily for the initial 2 weeks to gather a minimum of 10 measurements with the mean with the upper and lower limit (±2SD or standard deviation) with coefficient of variation ≤10% between Rrs in the two oscillometry devices in our laboratory. On August 30, 2021, we observed a BioQC measurement that fell outside the individual's mean ±2SD. The individual's observed R5 was 3.36 cmH2O·s/L (open circle), while R5 mean from the 20 most recent recordings was 4.95 cmH2O.s/L ±2SD (dotted line with lower limit at 4.03 and upper limit at 5.86; Figure 4). A second individual conducted their BioQC oscillometry on the same day with the same oscillometry device, and the observed R5 measurement was also outside the mean ±2SD. These findings indicate problems related to the instrument rather that than the procedure. Subsequently, the manufacturer was contacted and the device was sent for repair. Upon return of the device, BioQC was repeated on October 15, 2021 to ensure it was within the individual's R5 measurement range prior to redeployment of device in our laboratory.
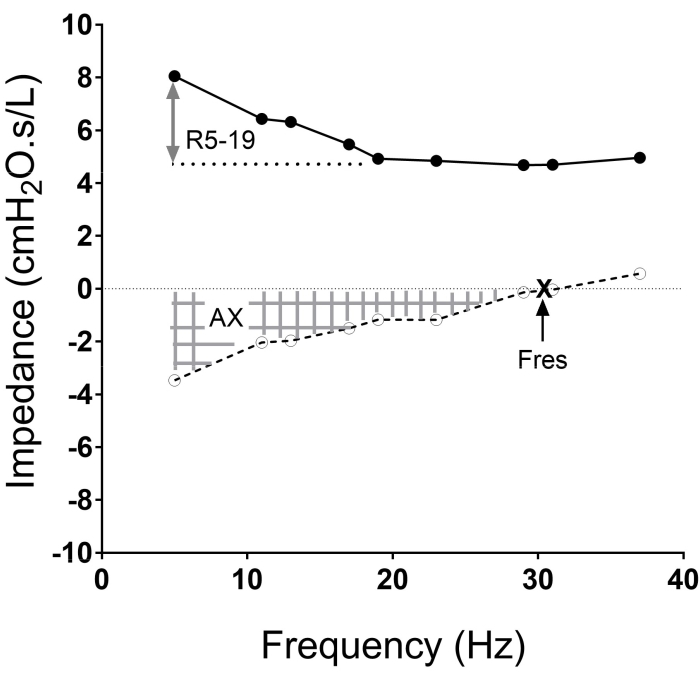
Figure 1: The impedance versus frequency oscillogram with the resistance curve (solid line) and reactance curves (dotted line), and frequencies at which the measurements are made (solid and open circles in each curve) shown. The area of reactance (AX, hatched area), resonant frequency (Fres. X), and resistance between 5 Hz to 19 Hz (R5-19; two-sided arrow) are illustrated. Please click here to view a larger version of this figure.
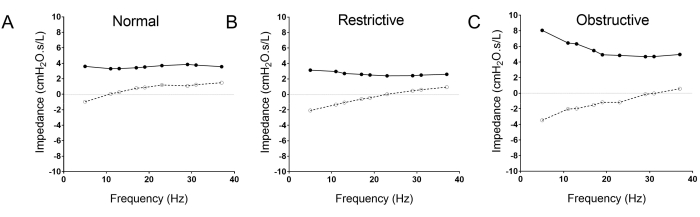
Figure 2: The typical oscillometry pattern differences between normal (A), restrictive (B) and obstructive (C) lung diseases. Note the rightward shift of the reactance curve (open circle, dotted line) in the restrictive disease (B), and the trumpet shaped pattern of the obstructive oscillogram (C) with upward shift of the resistance curve (solid circle and line), increased R5-19, and the downward and rightward shift of the resistance curve (broken line; open circles). Please click here to view a larger version of this figure.
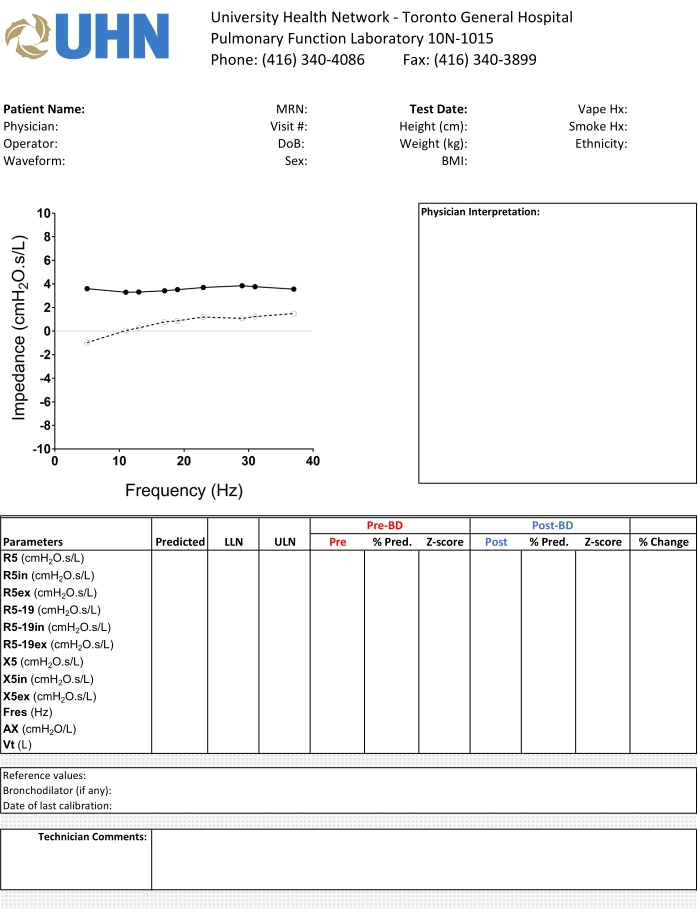
Figure 3: The standard template for reporting of oscillometry in our institution. We display the oscillogram using a standardized X-Y axis, and highlight the relevant pre- and post-bronchodilator measurements in different colors to facilitate interpretation of the results. Please click here to view a larger version of this figure.
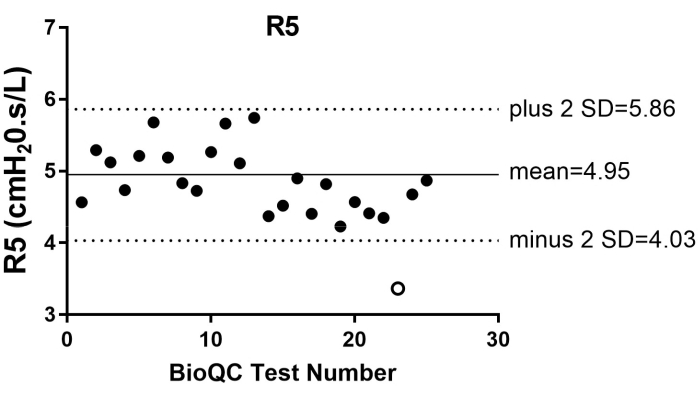
Figure 4: The biologic quality control (BioQC) summary of R5 measurements from one individual from May 2020 to November 2021. The measurement that fell outside (open circle) the individual's mean (solid grey line) ±2SD (dotted line) was observed in August 30, 2021. Please click here to view a larger version of this figure.
| First Audit | Second Audit | Third Audit | |
| October 17, 2017 to April 6, 2018 | April 9, 2018 to June 30, 2019 | July 2, 2019 to March 12, 2020 | |
| Valid | 187 | 1927 | 1770 |
| Invalid | 10 | 3 | 9 |
Table 1: Comparison of oscillometry tests acceptability at three time-points
Personnel underwent refresher training in conduct of oscillometry following the first audit. We also implemented a standard operating protocol for conduct of oscillometry in the pulmonary function laboratory. Significant improvements in the percentage of tests meeting acceptable quality control occurred and were sustained over time. These results demonstrate the effectiveness of developing and adhering to standard operating protocols and quality control guidelines.
Supplemental Table 1. Contraindications for Spirometry53,54 Please click here to download this Table.
Supplemental Table 2. Bronchodilators Withholding Times for Pulmonary Function Tests53,54 Please click here to download this Table.
Supplemental Table 3. Bronchodilators Withholding Times for Bronchial Challenge Test53,55 Please click here to download this Table.
