The current protocol results in a combination of objective and semi-subjective data, and the positive outcome depends on the accurate and repeatable assessment of specimens. Multiple observers with knowledge of the normal anatomy of the target species and an understanding of general dental and maxillofacial pathology ideally must be present to assess each specimen to minimize bias systematically. The assessment of each specimen must be discussed, and a consensus needs to be obtained. No threshold for the number of specimens has been suggested to ensure a representative sample, but published studies have included 76 to 1,205 individuals11,20. Additionally, a specimen free of any detectable pathology or minimal disease or anatomic variation must be found and documented to act as a standard for comparison (Figure 7). Furthermore, a successful outcome depends on the differentiation of pathology from artifactual damage. Often, specimens may incur artifactual damage during processing or storage. For this reason, for accurate data collection, the researcher must familiarize themselves with the general anatomy and pathophysiology of the maxillofacial region to understand the evidence of true chronic and acute disease processes. If there is evidence supporting that a finding is artifactual, such as evidence of post-mortem tampering with human tools or injuries to teeth or structures that would be biomechanically impossible in life, these findings must not be recorded as true pathology. If radiographs are utilized for specimen assessment, appropriate radiographic views need to be obtained for diagnostic quality38,39. Finally, pathology and anatomic anomalies must be documented with precise descriptions and/or high-resolution photographs.
Results may not be representative if normal anatomy is interpreted as pathology or if data are noted to have a high degree of variation between observers. Specimens must be examined carefully to preserve their quality as diligently as possible to allow for accurate repeat assessment in the future if necessary. Additionally, if meticulous record-keeping is not maintained, pathology or anatomical anomalies may be assigned to incorrect specimens, and the conclusions drawn from correlations from the data will be of questionable accuracy.
Data should be statistically analyzed to determine if there are differences in the frequency of abnormalities associated with the age of the individual at the time of death and sex. The frequency of dental abnormalities can be compared between different subspecies, geographic locations, and historic time points. Finally, data can be compared with previously published data on species of different genera.
The current protocol has proven to be an effective means of characterizing dental and TMJ abnormalities in various species11,12,13,14,15,16,17,18,19,20,21,22,23,24. The presentation of the results of future reports must follow a similar pattern to that of the previous manuscripts to maintain the completeness and to be able to compare results easily.
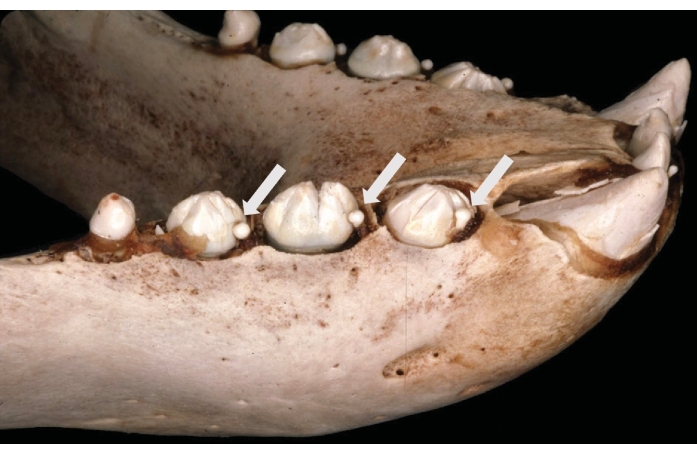
Figure 1: Persistent deciduous teeth in the Northern elephant seal (Mirounga angustirostris). Shown are persistent deciduous right mandibular first, second, and third premolar teeth (arrows) mesial to the corresponding permanent successor teeth. This figure has been modified from Abbott et al.12. Please click here to view a larger version of this figure.
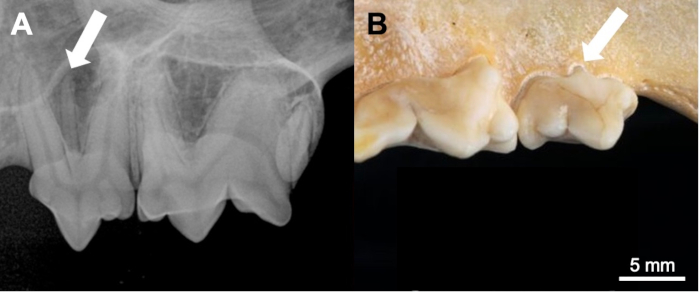
Figure 2: Supernumerary roots in the California bobcat (Lynx rufus californicus). (A) Radiographical and (B) gross appearance of a left maxillary third premolar tooth with an extra root (arrowed). This figure has been modified from Aghashani et al.19. Scale bar = 5 mm. Please click here to view a larger version of this figure.
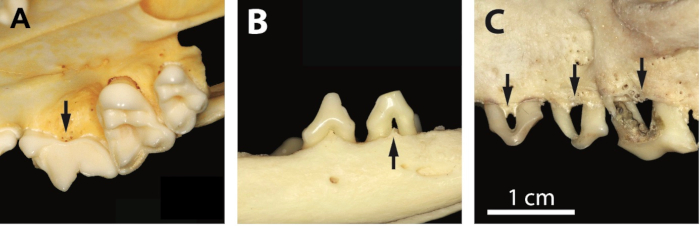
Figure 3: Stages of periodontitis in the grey fox (Urocyon cinereoargenteus). (A) Stage 2 associated with the right maxillary fourth premolar tooth, characterized by increased vascularization of the alveolar bone (arrow). (B) Stage 3 associated with the right mandibular second premolar tooth, characterized by moderate bone loss and furcation involvement (arrow). (C) Stage 4 associated with the left maxillary premolar teeth, characterized by severe alveolar bone loss (arrows). This figure has been modified from Evenhuis et al.22. Scale bar = 1 cm. Please click here to view a larger version of this figure.

Figure 4: Fractured teeth in the Northern fur seal (Callorhinus ursinus). Root fractures of the right mandibular third and fourth premolar teeth (white arrows) and stage 2 periodontitis around the right mandibular first molar tooth (black arrow)13. Scale bar = 1 cm. Please click here to view a larger version of this figure.

Figure 5: Periapical lesions in the Southern seal otter (Enhydra lutris nereis). Periapical disease associated with complicated crown root fractures of the right mandibular fourth premolar and first and second molar teeth in an adult female specimen. This figure has been modified from Winer et al.24. Please click here to view a larger version of this figure.
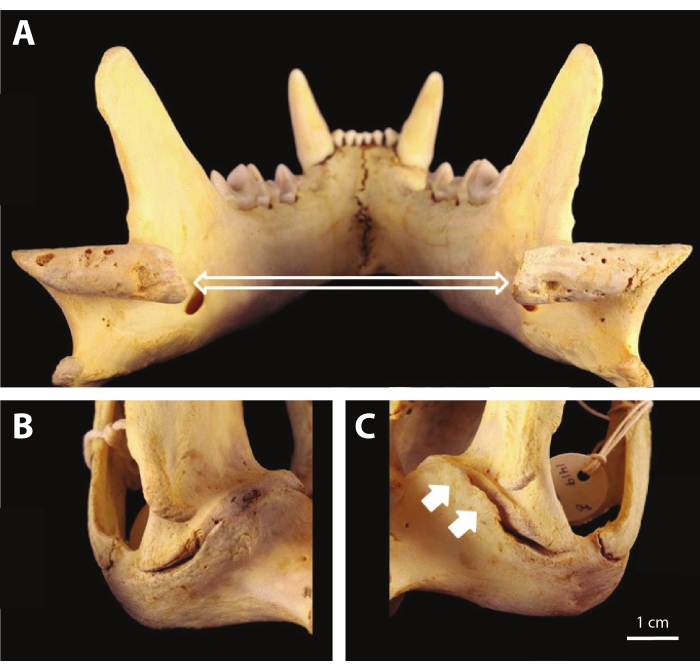
Figure 6: TMJ osteoarthritis in the California mountain lion (Puma concolor cougar). (A) Image of the irregular articular surface, subchondral bone exposure, and porosity of the mandibular condylar processes (open arrows). (B) The right TMJ exhibits no significant periarticular proliferation at the retroarticular process. (C) The left TMJ exhibits periarticular bony proliferation at the retroarticular process (closed arrows), partially encircling the mandibular head, resulting in partial ankylosis. This figure has been modified from Aghashani et al.21. Scale bar = 1 cm. Please click here to view a larger version of this figure.
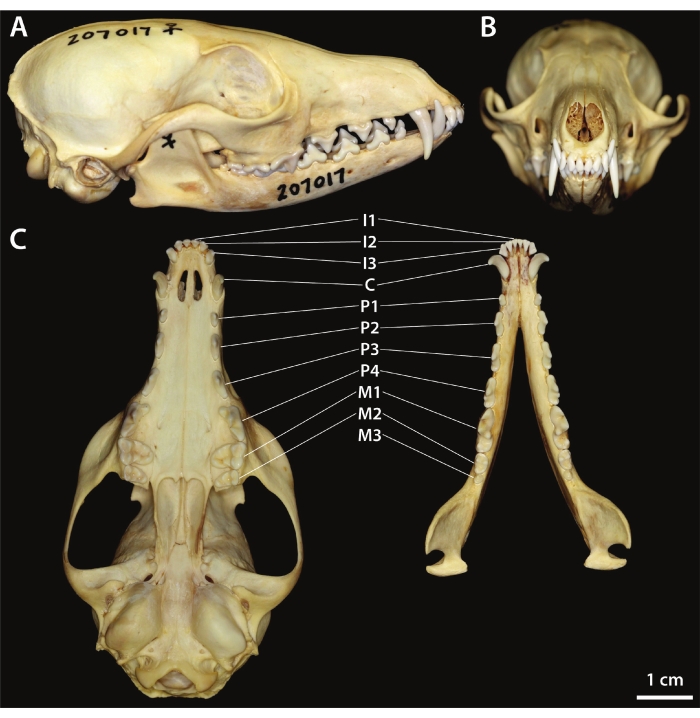
Figure 7: Normal dentition of the kit fox (Vulpes macrotis). (A) Right lateral view. (B) Rostral view. (C) Ventral view of the maxilla (left) and dorsal view of the mandibles (right). This figure has been modified from Yanagisawa et al.23. Scale bar = 1 cm. Please click here to view a larger version of this figure.
| Degree of Periodontitis | Clinical Features | ||
| Periodontitis stage 2 | Evidence of increased vascularity at the alveolar margin (more prominent vascular foramina in, and slightly rougher texture of, the bone of the alveolar margin) | ||
| Periodontitis stage 3 | Rounding of the alveolar margin; moderate horizontal or vertical bone loss | ||
| Periodontitis stage 4 | Widening of the periodontal space; severe horizontal or vertical bone loss; tooth mobile in the alveolus; furcation exposure | ||
Table 1: Summary of clinical features of progressive stages of periodontitis.
| Fracture Type | Description | |
| Enamel fracture | A chip fracture or crack of the enamel only. | |
| Uncomplicated crown fracture | A fracture involving enamel and dentine, but not exposing the pulp. | |
| Complicated crown fracture | A fracture involving enamel and dentine, with pulp exposure. | |
| Uncomplicated crown–root fracture | A fracture involving enamel, dentine and cementum, but not exposing the pulp. | |
| Complicated crown–root fracture | A fracture involving enamel, dentine and cementum, with pulp exposure. | |
| Root fracture | A fracture affecting dentine, cementum and the pulp. | |
Table 2: Summary of clinical features of tooth fracture types.
| Stage of Attrition/abrasion | Description | |
| Attrition/abrasion stage 1 | Mild wear of enamel, without dentine exposure | |
| Attrition/abrasion stage 2 | Exposure of dentine on the cuspal tip, without tertiary dentine formation | |
| Attrition/abrasion stage 3 | Exposure of dentine on the cuspal tip, with tertiary dentine formation | |
| Attrition/abrasion stage 4 | Pulp cavity exposure secondary to attrition/abrasion | |
Table 3: Summary of clinical features of tooth attrition and abrasion.
| Severity of Osteoarthritis (OA) | Clinical Features | ||
| Mild OA | There is any evidence of early lesions of periarticular new bone formation/osteophytes with minimal or no subchondral bone changes. | ||
| Moderate OA | There is periarticular new bone formation and/or subchondral bone changes are more pronounced. | ||
| Severe OA | All previously described signs are present and more pronounced, or if subchondral bone lysis is present. Partial or complete ankylosis may be observed. | ||
Table 4: Summary of clinical features of TMJ osteoarthritis.
