For the quantitative evaluation, two evaluation metrics were adopted, which were used in the CT image segmentation task. These were two similarity metrics, including dice score (DICE) and volume similarity (VS)13:
DICE (%) = 2 × TP/(2 × TP + FP + FN)
VS (%) = 1 − |FN − FP|/(2 × TP + FP + FN)
where TP, FP, and FN denote the true positive, false positive, and false negative values, respectively, when the segmentation result and the segmentation mask are given.
The performance of SEQ-UNET for orbital structure segmentation was evaluated by four cross-validations. The results are shown in Table 1. The eyeball segmentation using SEQ-UNET achieved a dice score of 0.86 and a VS of 0.83. The segmentation of the extraocular muscles and optic nerve achieved low dice scores (0.54 and 0.34, respectively). The dice score of the eyeball segmentation was over 80% because it had a large portion of the VOIs and little heterogeneity between CT scans. The dice scores of the extraocular muscles and optic nerve were relatively low because they infrequently appeared in the CT volume and were found in a relatively small number of the CT slices. However, the visual similarity scores of the extraocular muscles and optic nerve (0.65 and 0.80, respectively) were higher than their dice scores. This result indicates that the specificity of segmentation was low. Overall, the dice score and visual similarity of SEQ-UNET for the segmentation of all the orbital substructures were 0.79 and 0.82, respectively. Examples of the visual results of orbital structure segmentation are shown in Figure 3. In Figure 3A–C, blue is the predicted segmentation result, and red is the ground truth mask. In Figure 3D, red, green, and orange are the eyeball, optic muscle, and nerve segmentation, respectively.

Figure 1: Semi-automatic masking features. Masking the eyeball, extraocular muscles, and optic nerve on orbital CT scans using (A) SmartPencil, (B) SmartFill, and (C) AutoCorrection. The mask of the eyeball is labeled by SmartPencil, which computes the super pixels of the slices, and the mask is made by clicking on the super pixels. After clicking some of the eyeball super pixels, the entire eyeball mask can be computed by SmartFill. In the case of masking the optic nerve, the masking refinement is made by AutoCorrection. Blue color labeled eyeballs are shown in (A) and (B). Please click here to view a larger version of this figure.
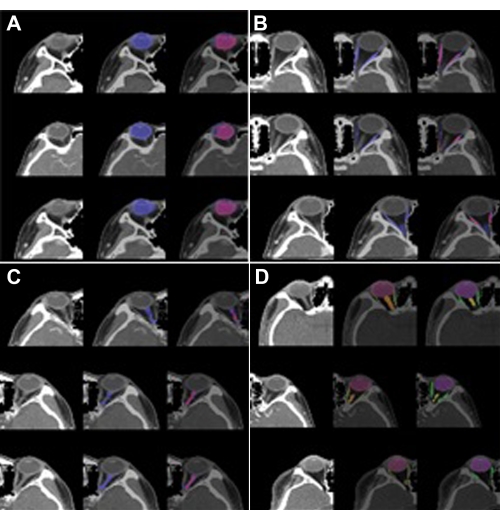
Figure 2: SEQ U-Net architecture. Sequential 2D slices as input and output; two bi-directional C-LSTMs are applied to the end of the encoding and decoding blocks based on the U-Net architecture. Please click here to view a larger version of this figure.
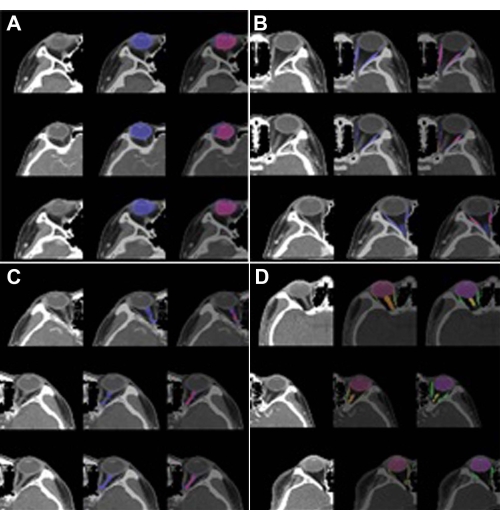
Figure 3: Segmentation results of the orbital structures. (A) Eyeball (label 1), (B) optic muscle (label 2), (C) optic nerve (label 3), and (D) multi-label (labels 1, 2, and 3). The left image is the VOI of the orbit, the center image is the predicted segmentation, and the right image is the ground truth. In (A), (B), and (C), blue is the predicted segmentation result, and red is the ground truth mask. In (D), red, green, and orange are the eyeball, extraocular muscle, and optic nerve segmentation, respectively. The predicted segmentation showed high performance (DICE: 0.86 vs. 0.82) in the case of the eyeball but low performance in the case of theextraocular muscle (DICE: 0.54 vs. 0.65) and optic nerve(DICE: 0.34 vs. 0.8). Please click here to view a larger version of this figure.
| Multi-Label | Label 1 (Eyeball) | Label 2 (Extraocular muscle) | Label 3 (Optic nerve) | |||||
| DICE | VS | DICE | VS | DICE | VS | DICE | VS | |
| SEQ-UNET | 0.79 | 0.82 | 0.86 | 0.83 | 0.54 | 0.65 | 0.34 | 0.8 |
Table 1: Segmentation results for the dice score and visual similarity. The eyeball, which has a relatively large number of slices, was segmented well with a DICE of 0.8, but the extraocular muscle and optic nerve, which have small numbers of slices and line shape, were partially segmented with DICE values of 0.54 and 0.34, respectively.
Video 1: SmartPencil wizard in the masking software program. A demonstration of annotating multiple pixels for eyeball masking. The masking tasks are enabled with one click on clustered super pixels. Please click here to download this Video.
Video 2: SmartFill wizard in the masking software program. A demonstration of annotating multiple pixels for eyeball masking. After selecting some pixels in the annotating area, this function generates full segmentation masks with similar intensities to the selected pixels. Please click here to download this Video.
Video 3: AutoCorrection in the masking software program. A demonstration of the automatic correction of a masked pixel using a pre-trained convolutional neural network algorithm. Please click here to download this Video.
Supplementary Table 1: Runtime environment (RTE) of masking, pre-processing, and segmentation modeling. Please click here to download this Table.
