Femoral anteversion can be measured by different methods. Some of them focus on the femoral neck, using the line passing through the center of the neck and one passing through the femoral condyles as references. Others add a third reference point at the lesser trochanter23. Murphy's method, which is the most reliable in clinical practice because it has the best clinical-radiological relationship, is one such method using a third reference point25,26. In addition, the torsional component of the femur, which varies in the different segments of the bone, contributes to the calculation of the FAV24.
In a preliminary study, the FAV was measured in 10 3D biomodels using Murphy's method 12. Then, a 10°, 20°, and 30° intertrochanteric rotational femoral osteotomy was simulated on each of the 3D biomodels (Group I). Once the osteotomy was performed, the FAV was remeasured, and it was observed that the rotation axis of the femur did not coincide with the rotation axis of the osteotomy in group I.
Through the 3D guides, one can see that the two axes do not coincide because the red guide does not match the violet guide (3D Builder, Supplementary File 1). The red guide represents the rotational axis of the osteotomy, while the violet guide represents the rotational axis of the femur. For this reason, it is necessary to make an adjustment that involves realigning the two guides so that the rotation axis of the femur and the rotation axis of the osteotomy coincide (3D Builder, steps 4.8.1-4.8.3, Supplementary File 1) (Figure 1).
Therefore, another surgical simulation of the osteotomy was performed, and a reset was needed to match the axis of femoral rotation with the rotation axis of the osteotomy. The resulting FAV was measured again (Group II). Table 1 details the values of the FAV obtained in each group for the three magnitudes of rotational osteotomy (10°, 20°, and 30°). The variable"correction" was defined as the difference between the initial FAV and the FAV measured after the osteotomy. When the adjustment was made so that the femur's rotation axis and the osteotomy's rotation axis coincided, the relationship between the planned correctionand the final correction was 1:1 in the three correction magnitudes(10°, 20°, and 30°) (Table 2). The same did not occur in group 1, inwhich the 1:1 ratio was not achieved (Table 2).
| Group 1 | Group 2 | P value | |
| FAV 10° | 22° (±9.1º) | 17.9° (±8.8º) | <0.001 |
| FAV 20° | 15.8° (±8.7º) | 7.7° (±9.6º) | <0.001 |
| FAV 30° | 8.9° (±8.9º) | -2.2° (±10.3º) | <0.001 |
Table 1: FAV comparison between Group 1 and Group 2. The means and SD values are presented. Abbreviation: FAV = femoral anteversion.
| Derotation (correction) | Group 1 | Group 2 | P value |
| 10° | 6.9° (±1.4º) | 11.1° (±2.8º) | <0.001 |
| 20° | 13.1° (±3.2º) | 21.3° (±6.0º) | <0.001 |
| 30° | 20° (±5.1º) | 31.3° (±8.3º) | <0.001 |
Table 2: Correction comparison between group 1 and group 2. The means and SD values are presented.
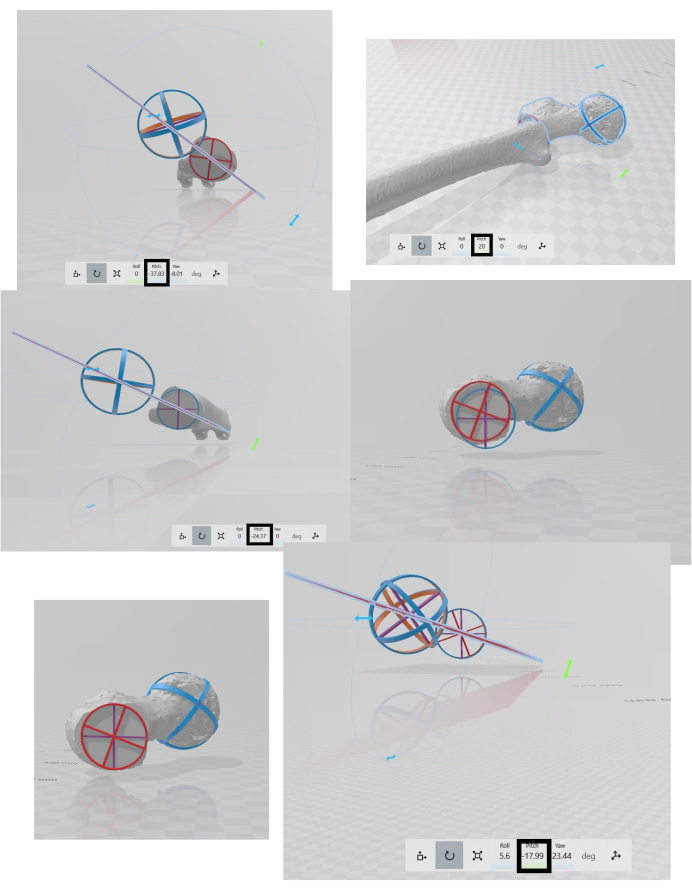
Figure 1: The final outcome: The result of the osteotomy after the adjustment has been applied. There are six panels, which should be read from left to right and from top to bottom. First panel: femoral anteversion calculated in the CT using Murphy's method. Second panel: Rotational osteotomy of the proximal femur (internal rotation of 20°). Third panel: New femoral anteversion after the rotational osteotomy of the proximal femur (the final correction does not coincide with the planned correction). Fourth panel: The guides do not match. Fifth panel: Matching the guides. Sixth panel: New femoral anteversion with the adjustment made (the final correction coincides with the planned correction). Please click here to view a larger version of this figure.
Supplementary File 1: Software instructions. The 3D Slicer software (obtaining and creating the biomodel); the MeshMixer software (making the solid model); the 3D Builder software (importing the biomodel, performing the femoral osteotomy, and calculating the femoral anteversion). Please click here to download this File.
Supplementary File 2: Osteotomy guides. A 3mf file containing the red circular guide, purple circular guide, sphere, and red plane (https://www.dropbox.com/work/JoVE%20Review/File%20requests/64474?preview=Guides+osteotomy+Caterina+Chiappe.3mf).
