The presented model has been successfully used in several experiments to study macrocirculatory and microcirculatory changes following hemorrhagic shock and subsequent resuscitation, comparing different fluids and vasoactive drugs16,17,18,19.
Considering the response to shock, this model has consistently shown that a controlled hemorrhage produces marked changes in hemodynamic parameters, as well as in cerebral and tissue perfusion.
Following volume withdrawal, significant tachycardia and a decrease in MAP, CI, SVI, blood volume parameters (GEDVI and ITBI), and carotid arterial blood flow, along with an increase in systemic vascular resistance index, are detected (Figure 1 and Figure 2).
Regarding systemic perfusion parameters, lactate increases significantly, whereas ScvO2, CuTBF, and bTO decreases (Figure 3). Variations in central venous pressure, Dt/Dpmax, and ELWare not usually registered.
As for laboratory parameters, hemoglobin content and hematocrit do not decrease until after fluids have been administered. Albumin concentration decreases, and troponin levels increase significantly after controlled hemorrhage. Other parameters, including core temperature, PaO2, PaCO2, arterial oxygen saturation, EtCO2, electrolytes, and kidney and liver function parameters, usually remain stable.
Besides its utility in analyzing the cardiovascular and biochemical responses to shock, this model has been shown to successfullydiscriminate between different resuscitation fluids.
In previous studies, we have aimed to determine if, in an infant animal model of hemorrhagic shock, the use of a lower volume infusion of hypertonic fluids-alone or combined with different vasopressors- would improve global hemodynamic and perfusion parameters when compared to normal saline.
As reported previously, we have consistently observed that the infusion of hypertonic fluids produces a similar response to the infusion of twice the volume of isotonic fluid16,17,18.
More specifically, the use of albumin plus hypertonic saline produced a greater and longer volume expansion than normal saline or hypertonic saline alone, with significant differences in HR, SVI, and PPV, and the absence of a progressive fall after volume expansion in blood pressure and GEDVI, as observed in the other groups (Figure 1 and Figure 2). Furthermore, we have also observed a greater improvement of perfusion parameters with hypertonic albumin, represented as a greater increase of bTOI and CaBF, and a greater decrease of lactate levels than the other groups in comparison with the beginning of the fluid expansion (Figure 3). We believe that this difference might be secondary to the capacity of albumin to increase the blood volume and remain for a longer period of time within the intravascular compartment than normal saline.Interestingly, we have seen that the addition of a single bolus of terlipressin at the beginning of fluid resuscitation yielded similar results to those observed in the hypertonic albumin group, without any extra benefits in terms of hemodynamic or perfusion parameters17,18.
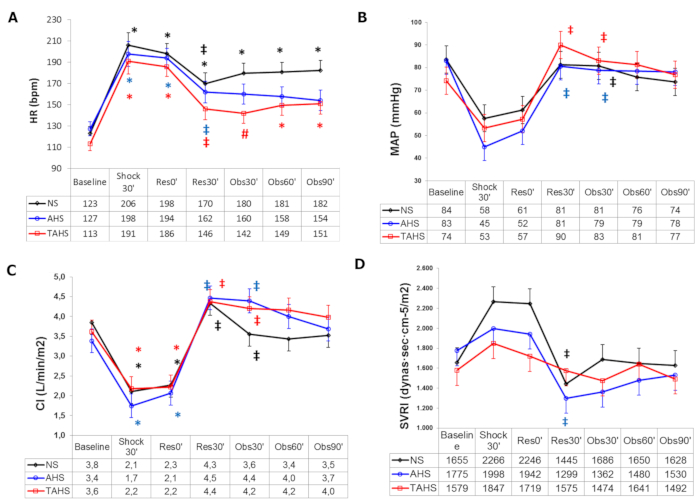
Figure 1: Hemodynamic parameters. (A) Evolution of heart rate, (B) mean arterial pressure, (C) cardiac index at baseline (t0'), and (D) systemic vascular resistance index at baseline (t0'). Throughout the course of the experiment: end of controlled bleeding (Shock30'); the beginning of infusion, 30 min after the end of controlled bleeding (Res0'); end of infusion (Res30'); follow-up 30 min after the end of infusion (Obs30'); follow-up 60 min after the end of infusion (Obs60'); follow-up 90 min after the end of infusion (Obs90'). (*) Significant difference (p < 0.05) from the baseline, same group. (‡) p < 0.05 from hemorrhage, same group. (#) p < 0.05 from group NS. Abbreviations: NS = normal saline; AHS = hypertonic saline albumin; TAHS = terlipressin plus hypertonic saline albumin. Data are presented as mean and standard deviation. This figure is adapted with permission from Urbano et al.17. Please click here to view a larger version of this figure.
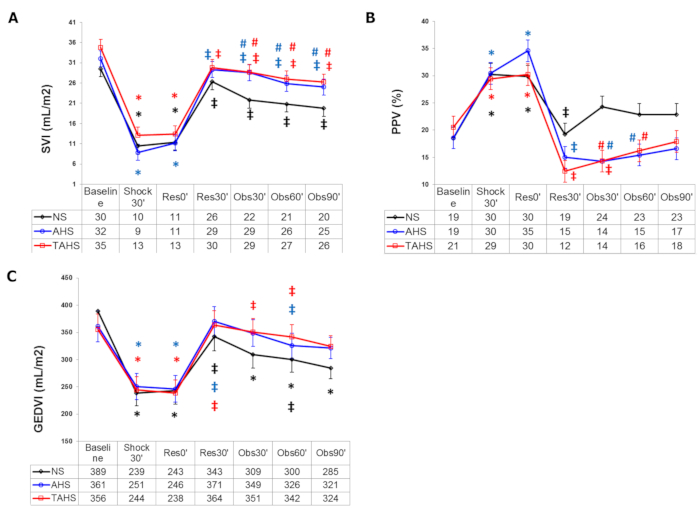
Figure 2: Blood volume parameters. (A) Evolution of stroke volume index, (B) pulse pressure variation, and (C) global end diastolic volume index at baseline (t0'). Throughout the course of the experiment: end of controlled bleeding (Shock30'); beginning of infusion, 30 min after the end of controlled bleeding (Res0'); end of infusion (Res30'); follow-up 30 min after the end of infusion (Obs30'); follow-up 60 min after the end of infusion (Obs60'); follow-up 90 min after the end of infusion (Obs90'). (*) Significant difference (p < 0.05) from baseline, same group. (‡) p < 0.05 from hemorrhage, same group. (#) p < 0.05 from group NS. Abbreviations: NS = normal saline; AHS = hypertonic saline albumin; TAHS = terlipressin plus hypertonic saline albumin. Data are presented as mean and standard deviation. This figure is adapted with permission from Urbano et al.17. Please click here to view a larger version of this figure.
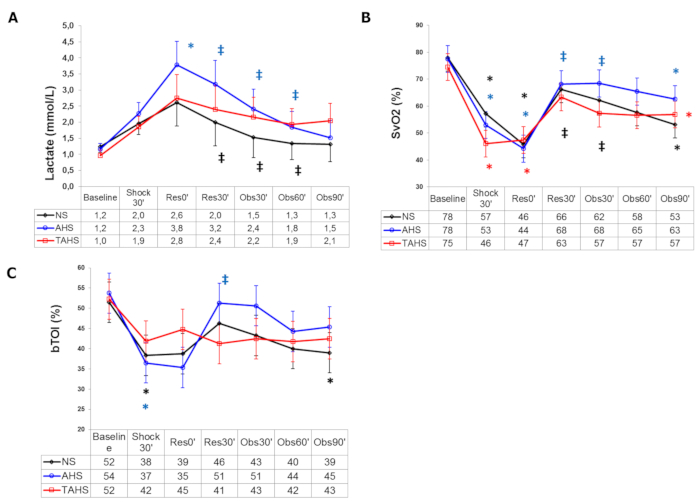
Figure 3: Systemic perfusion parameters. (A) Evolution of arterial blood lactate, (B) central venous blood oxygen saturation, and (C) brain tissue oxygenation index at baseline (t0'). Throughout the course of the experiment: end of controlled bleeding (Shock30'); beginning of infusion, 30 min after the end of controlled bleeding (Res0'); end of infusion (Res30'); follow-up 30 min after the end of infusion (Obs30'); follow-up 60 min after the end of infusion (Obs60'); follow-up 90 min after the end of infusion (Obs90'). (*) Significant difference (p < 0.05) from baseline, same group. (‡) p < 0.05 from hemorrhage, same group. (#) p < 0.05 from group NS. Data are presented as mean and standard deviation. This figure is adapted with permission from Urbano et al.17. Please click here to view a larger version of this figure.
