Figure 1 and Figure 2 show the materials needed for the experiment, and Figure 3 displays the sequential steps and the successful mid-products during the preparation of mACS. First, 0.5 mL of 10% glycerol solution was added into each 10 mL sterile test tube (Figure 3A). Then, 60-70 mL of venous blood was obtained from the patient, and 10 mL of blood was injected into each tube (Figure 3B). The patient's blood must be subjected to thorough, regular laboratory examinations before the preparation to ensure that the quality of the blood is up to standard. The most common low-quality blood product is due to dyslipidemia, which results in a cloudy upper layer of serum after centrifugation that is difficult to remove; further preparation of eye drops cannot be continued (Figure 5A).
Then, the sealed test tube is placed in an incubator at 37 °C for 4 h (Figure 3C). After incubation and centrifugation, the sample could be separated into an upper layer containing the preliminary product of mACS and a lower blood cell layer (Figure 3D). The upper layer fluid was then collected. Aseptic techniques are essential hereafter. Because the serum is a very nutritious breeding environment for microorganisms, any surface that comes into contact with the needle must be disinfected with 75% alcohol first, and sterile gloves must be used during the process. Importantly, disturbance of the blood cells from the lower layer should be avoided when removing the supernatant (Figure 3E).
At this step, it is expected that the supernatant is clear or pale yellow. However, if a slight red color is seen, hemolysis may have occurred, and the preparation may not be suitable for the subsequent steps (Figure 5B). The collected serum could be centrifuged again to ensure the supernatant is free of red blood cells. The serum was filtered through a 0.22 µm filter into a sterile eye drop bottle (Figures 3F,G). The final product, mACS eye drops, was then refrigerated or frozen as soon as possible, depending on the purpose (Figure 3H). The eye drops could not be stored for too long because of their richness in labile nutrients and the lack of preservatives.
In the ex vivo surface healing model, the mACS eye drop showed a superior outcome in corneal wound healing compared with the AS eye drop. Harvesting the eyeballs of C57BL/6 mice was done after creating a concentric corneal wound by physical abrasion under the microscope. Then, the sacrificed mice eyes were cultured in four different media, including pure normal saline, DMEM, 0.5% AS, and 0.5% mACS.
The AS medium used here was prepared based on the literature21 and the clinical practice in Chang Gung Memorial Hospital Linkou. Venous blood, 40 mL in total, was drawn into vacutainer tubes from volunteers after skin sterilization. No anticoagulant was added to the tubes. The blood was then stored for 30 min at room temperature to ensure complete clotting followed by centrifugation at 3,500 × g for 10 min. After centrifugation, the pure AS occupied the upper layer of the tubes, which was diluted by BSS (sterile irrigating solution) to 0.5% in this ex vivo animal model.
Corneal wounds were sequentially observed at six different time points, namely 0, 8, 16, 24, 32, and 48 h. The preliminary results showed that, at 16 h, the corneal wounds healed faster under the 0.5% mACS eye drop than the other groups. At 24 h, the 0.5% AS and DMEM groups had comparable therapeutic effects with the 0.5% mACS eye drop. Healing of the corneal wounds, close to full recovery, was observed at 32 h, except for the normal saline group (Figure 4).
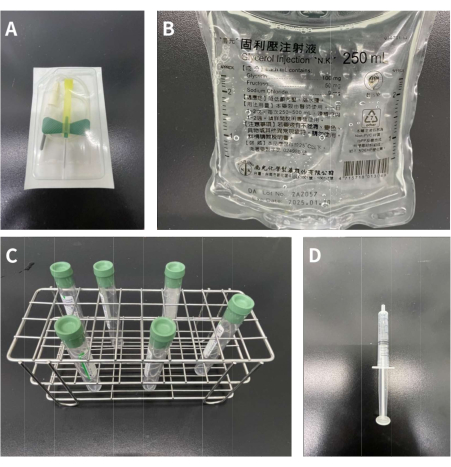
Figure 1: Materials needed for adding 10% glycerol solution into the tubes. (A) 21 G butterfly-winged infusion set. (B) 250 mL of 10% glycerol solution. (C) Six 10 mL vacutainer tubes containing heparin 158 USP units. (D) 3.0 mL syringe. Please click here to view a larger version of this figure.
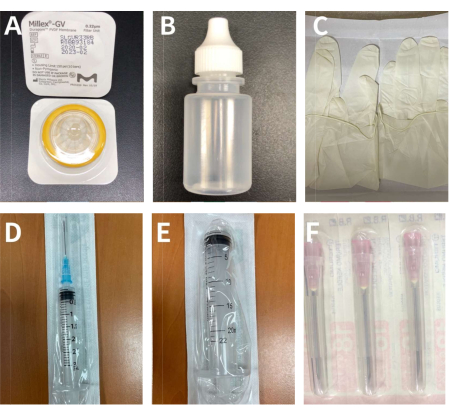
Figure 2: The materials for extraction and filtration of the supernatant of the blood sample. (A) A 0.22 µm filter. (B) A 5 mL sterilized eye drop bottle. (C) A pair of sterile gloves. (D) A 3 mL syringe with the 23 G needle. (E) A 20 mL syringe. (F) 18 G needles. Please click here to view a larger version of this figure.
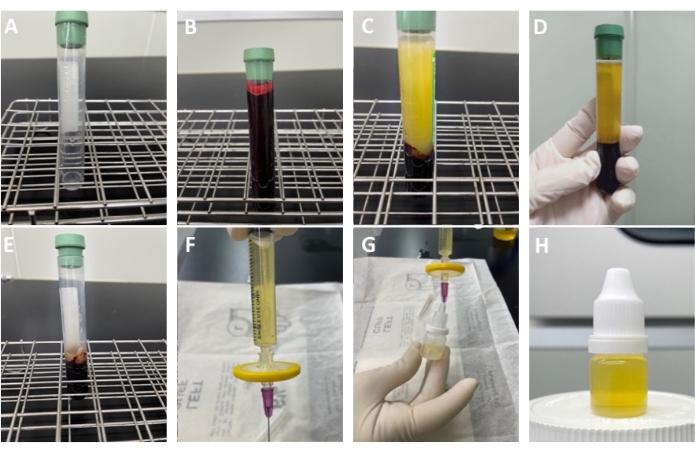
Figure 3: Procedures for blood centrifugation and preparation for the production of modified autologous conditioned serum eye drops. (A) 0.5 mL of 10% glycerol solution was added into each test tube. (B) The blood sample collected from the patient was divided equally into six test tubes (only one shown in the image). (C) Appearance of the test tube after being placed in a 37 °C incubator for 4 h. (D) The serum and blood cell layers after centrifugation. (E) The residue after aspirating the supernatant. One should be careful not to aspirate the lower blood cell layer. (F) The supernatant is collected in the 3 mL syringe and a 0.22 µm filter and 23 G needle are inserted below it. (G) The needle is gently pushed into the sterile eye drop bottle. (H) Final product of the modified ACS eye drops. Please click here to view a larger version of this figure.

Figure 4: Sequential changes of corneal wounds (green areas in the figures after fluorescein staining) in murine eyes in four different culture media over time. No significant difference was observed in the saline group, while wound healing (arrows) over time was observed in the DMEM, 0.5% AS, and 0.5% mACS groups. In the 0.5% mACS group, the wound healing (arrows) was significantly more complete at 16 h than those treated with AS and DMEM. At 24 h, the DMEM, 0.5% mACS, and 0.5% AS groups showed further healing effects (arrows), especially in the mACS group. Near total recovery was observed at 32 h for all groups, except for the saline group. Please click here to view a larger version of this figure.

Figure 5: Examples of poor blood products after centrifugation. (A) Dyslipidemia. The most common defective products are due to obesity or diabetes mellitus, as the upper serum contains high fat and cholesterol. (B) Hemolysis. This is also a common sub-optimal product. The main reason can be attributed to using small bore needles for blood drawing or using inappropriate external force in injecting blood products. Please click here to view a larger version of this figure.
