In order to confirm the placement (Figure 3A) and functionality of the devices, electrophysiological recordings are performed intraoperatively after pedestal placement. The baseline signal is first acquired over 2 min with no stimuli as the control of basal activity. Secondly, the animal is acoustically stimulated with a tone burst at different frequencies (500-20,000 Hz), and the raw data is averaged over the stimulus period to map auditory evoked potentials across the array (e.g., at 800 Hz compared to baseline; Figure 3B). The data shown here are unprocessed, but if too much noise is present, notch and bandpass filters can be applied. Typical sources of noise in the surgical theater include heating pads, plugged drills, and suction or cauterizers (among others) that should be removed prior to acquisition. In awake recordings, large muscle movement around the head, such as chewing, should be avoided for cleaner data sets.
This protocol was applied at every recording time point, and signals for a single channel could be compared over time. One example is illustrated in Figure 3C, showing the robustness and evolution of the response. The recording capacity of each contact over the time course of the experiment can be evaluated by calculating the standard deviation of the baseline signal at every time point (Figure 3D). In this study, the signal-to-noise ratio decreased and settled between day 0 and month 6, despite some variability due to the limited duration of the recording period (i.e., 2 min). This can be further correlated to electrode impedances.
The in vivo imaging is performed postoperatively to assess the brain state and implant positioning. In the first iteration of the protocol, no intraoperative x-ray was performed, resulting in a folded device, as is visible in Figure 4A on a T1-weighted MRI sequence (see in addition Figure 4B). No behavioral change was observed in the animal, but over time, this resulted in a fibrotic encapsulation around the device due to the macroscopic compression of the brain around the implant location (Figure 4C). After this experience, intraoperative x-ray was introduced, as shown in Figure 4D, where the radiopaque markers (black bars visible on the implant in inset Figure 4D) are shown to be well positioned. The surface of the brain is then intact, as can be observed in the postoperative MRI in Figure 4E. Overall, with this implant and pedestal system, whole-brain imaging is possible. Different sequences in the coronal planes enable to see anatomical structures (Figure 4F,G; T1 and T2 MRI sequences) or the presence of liquid and blood around the implant (Figure 4H; TSE-weighted MRI sequence). The pedestal system creates almost no artifacts, except for some small black-contrasted voids around the titanium screws (see Figure 4G). Additionally, clinical electrodes are used as comparators in this study, but cannot be imaged in the MRI due to heating and safety concerns. Therefore, CT scans are acquired on these animals, as shown in Figure 4I. The electrodes are clearly visible, and the pedestal system is not influencing the image quality.
After the implantation period, the animal is perfused, and the brain extracted. In this study, the analysis of the inflammatory response is performed on each hemisphere independently. Cutting the brain in half is easier for tissue preparation before sectioning, and has the advantage that sections can be mounted on standard microscopy slides. One example of a brain sample is shown before (Figure 5A) and after (Figure 5B) cutting in blocks. The outline of the implant is clearly visible and has created a small dent in the brain. By cutting in parallel planes, the tissue is then already aligned to the cryostat, and sections can readily be cut without tissue loss for trimming (Figure 5C). After staining, the whole tissue section is imaged (Figure 5D), where for example, the neuron layer is clearly visible in detail (see NeuN marker). Whole sections are fragile and can sometimes lead to some loss of tissue (see the bottom of Figure 5D), but the area of interest is intact. On a closer view, enabled by confocal microscopy imaging at 40x, the cells are clearly defined and enable fine investigation of inflammatory markers, for example (Figure 5E). Further quantifying analysis can be performed to compare inflammation between control and implanted hemispheres. Figure 6 shows the electrochemical characterization of the implanted electrodes. The In vitro electrochemical impedance spectroscopy of the soft electrode array with impedance modulus and phase is shown in Figure 6A and the impedance modulus at 1 kHz over 6 months of implantation is shown in Figure 6B.
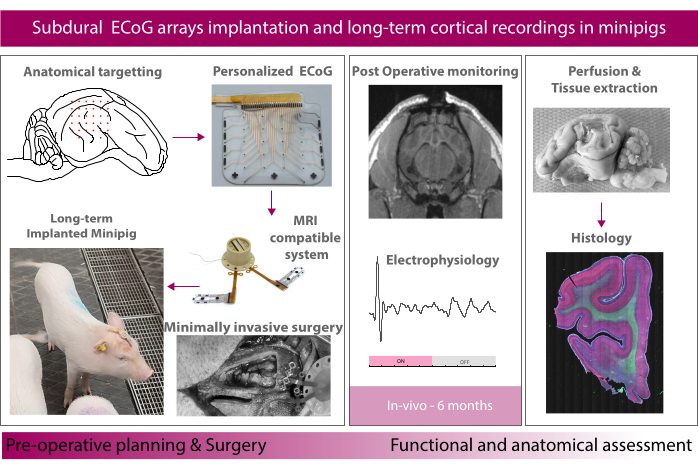
Figure 1: Schematic of the experiment. Please click here to view a larger version of this figure.
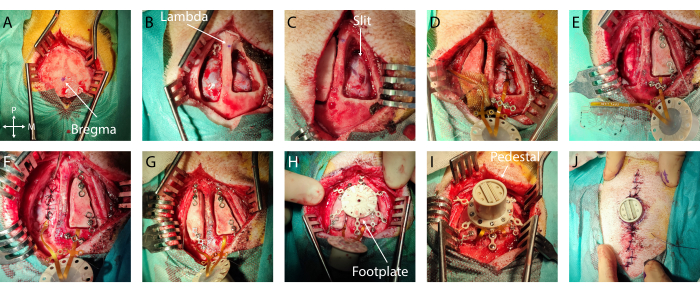
Figure 2: Minimally invasive implantation of soft ECoG onto the brain. (A) Surgical access to the skull, with indication of bregma. (B) Bilateral craniotomy with visible dura mater. (C) Slit durotomy on the first hemisphere. (D) Subdural implantation of soft ECoG and dura mater closure. (E) Slit durotomy on the second hemisphere. Bone flap fixation on the first hemisphere using titanium bridges. (F) Implantation of soft ECoG on the second hemisphere and dura mater closure. (G) Bone flap fixation on the second hemisphere. (H) Footplate positioning on the skull. (I) Pedestal fixation onto the footplate. (J) Skin closure around the pedestal base. Please click here to view a larger version of this figure.
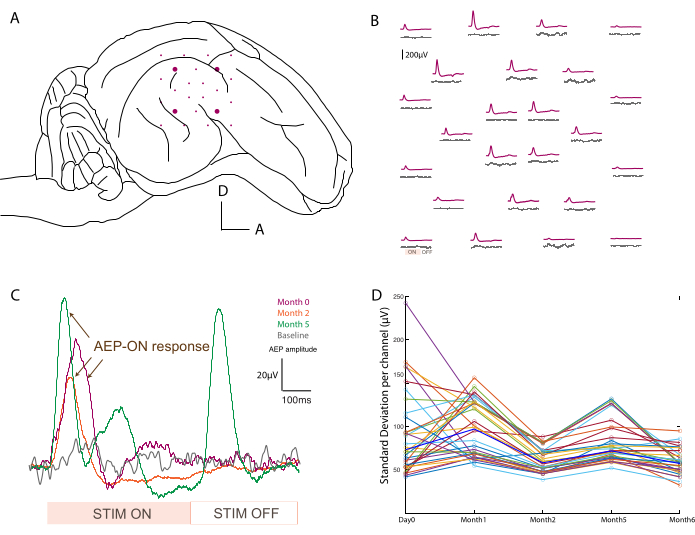
Figure 3: Recording of auditory evoked potentials. (A) Schematic of electrode placement at the surface of the temporal lobe. (B) Representative mapping of baseline activity (gray traces) and auditory evoked potentials in response to an 800 Hz tone burst stimulation (purple trace). Each average corresponds to one channel on the soft ECoG array. The averaging is triggered on the analog input signal from the sound stimulation. "ON" and "OFF" acoustic stimulation periods are noted on one channel in the bottom left. (C) Evolution over time (day 0, month 2, and month 5) of a single channel response after acoustic stimulus, compared to baseline signal when no stimulus is presented (gray). The averaging is triggered on the analog input signal from the sound stimulation. The "ON" and "OFF" stimulation periods are noted at the bottom. The evoked potential of the "ON" stimulation is marked with arrows. (D) Standard deviation per channel (colored dots) per time point of the baseline recording. Median values are represented in bold blue. Please click here to view a larger version of this figure.
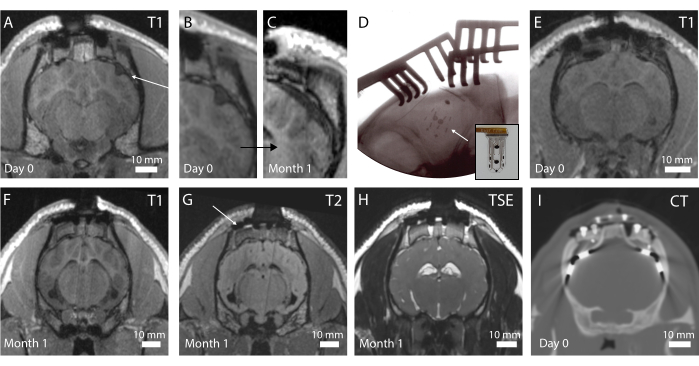
Figure 4: In vivo imaging of the brain and implanted electrodes. (A) Postoperative T1-weighted MRI in the coronal plane. An arrow indicates a folded implant. (B) Magnified portion of A, where the folding of the implant creates a dent in the brain. (C) T1-weighted MRI at 1 month implantation, showing compression of the brain due to the fibrotic encapsulation of the brain at the same location as C. (D) Intraoperative plane x-ray verifying implant placement and no folding, as observed by the radiopaque marker placement. Inset: Photograph of implant with radiopaque marker visible. (E) Postoperative T1-weighted MRI in the coronal plane with optimal implant placement. (F) T1-weighted MRI at 1 month implantation. (G) T2-weighted MRI at 1 month implantation. An arrow shows the imaging artifact from the titanium screws holding the footplate in place on the skull. (H) TSE-weighted MRI at 1 month implantation. (I) CT scan of the animal implanted with the clinical electrodes. Please click here to view a larger version of this figure.
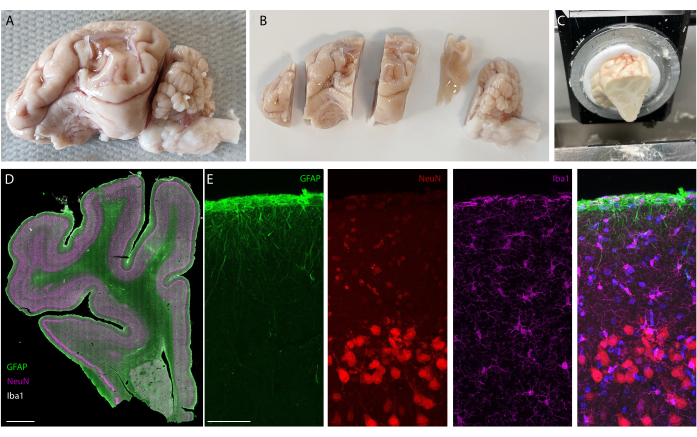
Figure 5: Histology analysis of the brain after long-term implantation. (A) Photograph of an explanted and perfused brain-left hemisphere. (B) Perfused brain cut in blocks prior to the freezing step. (C) Picture of whole block sectioning setup on the cryostat; the entire "pre-cut blocks" can be sectioned. (D) Immunostaining imaging of the whole hemisphere (slide scanner, 20x objective) and(E) zooming on the first layers of the cortex (confocal imaging, 40x objective) showing glial cells, astrocytes, and neurons. Please click here to view a larger version of this figure.
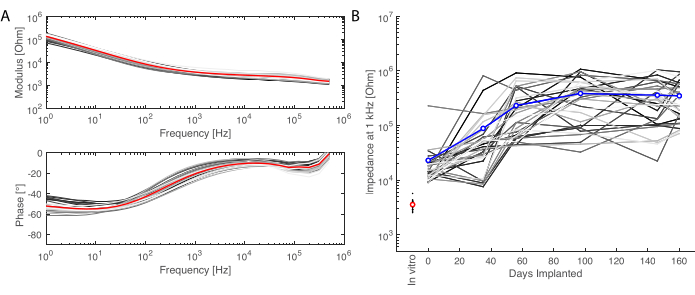
Figure 6: Electrochemical characterization of the implanted electrodes. (A) In vitro electrochemical impedance spectroscopy of the soft electrode array (small grey lines for each channel, the average in red) with impedance modulus (top) and phase (bottom). (B) Evolution of the impedance modulus at 1 kHz over 6 months of implantation (mean in blue; grey lines are the individual channels; the in vitro measurement is given as reference in red). Please click here to view a larger version of this figure.
Supplementary Figure 1: MRI-compatible pedestal. (A) Chronic MRI-compatible transdermal connection system (pedestal) to access the soft electrode array. (B) Pedestal with electrodes mounted on the footplate for skull anchoring. Inset: Details of the footplate. Please click here to download this File.
Supplementary Figure 2: Surgical access for optimal perfusion of the brain. (A) Skin cut and access to the location of the carotid artery and jugular vein. (B) Dissection of the tissue around the blood vessels. (C,D) Identification and dissection of the tissue around the carotid artery and jugular vein. (E) Isolation of the carotid artery from the tissue beneath. (F) Isolation of the jugular vein from the tissue beneath. (G) Suture wire placement around the carotid artery (suture 1 and suture 2) and the jugular vein (suture 3). (H) Closure of suture 3 at the base of the carotid artery (heart side) to avoid bleeding during opening of the vessel. (I) Clamping of the carotid artery at the opposite side from H. (J) Sectioning of the carotid artery. (K) Inserted catheter in the opening from J. Inset: Primed catheter with saline flushed from a syringe to the catheter tip. (L) Closure of suture 2 to maintain the catheter in place and along the artery. Please click here to download this File.
Supplementary File 1: Parameters for T1- (pages 1-2), T2- (pages (3-4) and TSE-weighted (pages 5-6) MRI sequences, respectively. Please click here to download this File.
Supplementary File 2: Metadata for slide scanner for whole slide imaging of stained brain slices. Please click here to download this File.
Supplementary File 3: Metadata for confocal imaging of magnified section of stained brain slices. Please click here to download this File.
