This investigation utilizes actual patient datasets acquired using a commercially available MRI scanner to validate the 3D liver fat fraction quantification methodology (Figure 1). The MRI protocol included Dixon's four-phase imaging9,10: In-phase, Out-of-phase, Water-only, and Fat-only (Figure 2). The fat fraction (FF) of each voxel is computed by dividing the In-phase minus Water-only voxel signal by the In-phase voxel signal using Dixon MRI. This numeric model allows accurate calculation of the fat content percentage in each voxel.
Although deep learning methods can extract 3D liver anatomy, they have inherent algorithmic errors. To ensure precise quantification, mature software tools like MIMICS were used to extract an accurate 3D liver contour combined with expert guidance (Figure 3).
Fusing the 3D liver contour with the 2D FF map in Figure 4 generates an integrated 3D-FF distribution model in Figure 5. This overcomes the limitation of 2D FF maps and provides visualization of fat deposition in the entire liver volume. Doctors can now accurately locate fat content in 3D liver space instead of a vague impression.
As Figure 6 shows, the 3D-FF distribution reveals fat fraction values at different liver positions. By comparing this to standard FF thresholds, the percentage of voxels falling into different stages of hepatic steatosis can be quantified. This enables precise measurement of the proportion of liver at various steatosis levels.
Comparison between a normal and fatty liver (Figure 7) validates the technique's ability to discern different 3D-LFF distribution patterns. The proposed workflow demonstrates clinical value in the 3D visualization, quantification, and diagnosis of hepatic steatosis based on patient's Dixon MRI data.
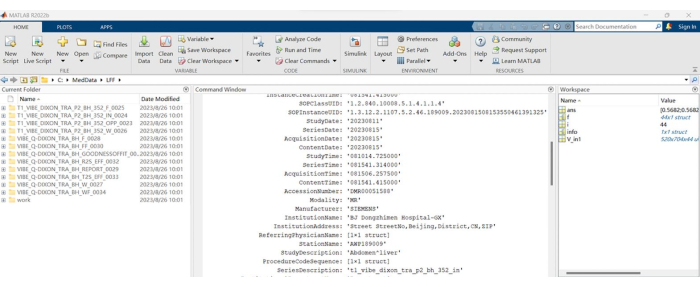
Figure 1: MRI-Dixon sequence folders. A list of folder names corresponding to the Dixon MRI scan sequences used in the study. Please click here to view a larger version of this figure.
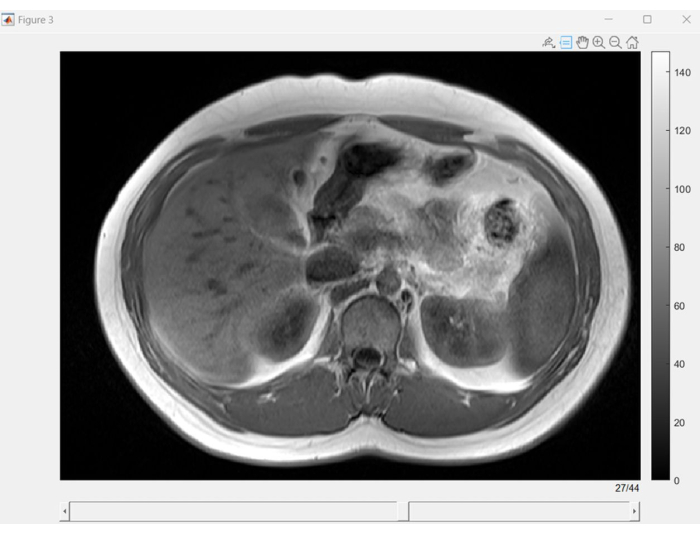
Figure 2: Dixon MRI slice browser. Graphical user interface (GUI) displaying slices from each phase sequence of Dixon MRI. Dixon MRI is valuable for enhancing image quality and interpretability, especially when precise fat and water separation is essential. Please click here to view a larger version of this figure.
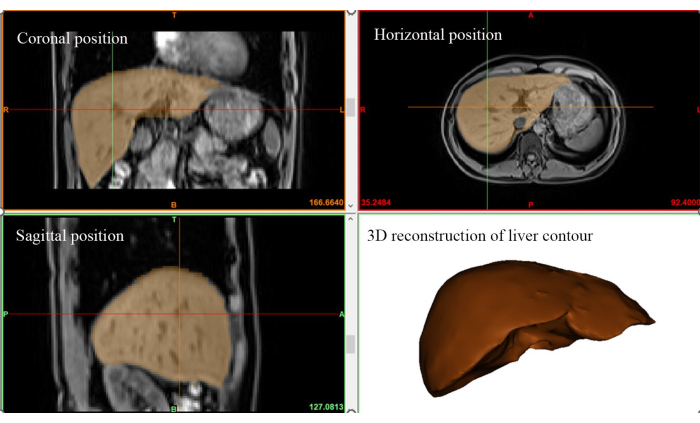
Figure 3: 3D liver region extraction. Visualization of the three-dimensional spatial extent of the liver based on In-Phase images acquired during the MRI scan. Please click here to view a larger version of this figure.
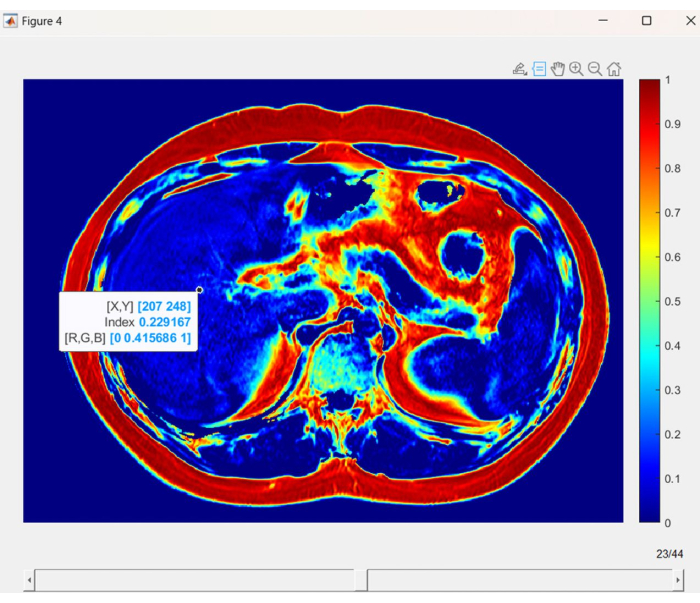
Figure 4: Liver fat fraction map. A visual representation of liver fat fraction (LFF) in each voxel, using distinct colors to indicate variations in fat content. Please click here to view a larger version of this figure.
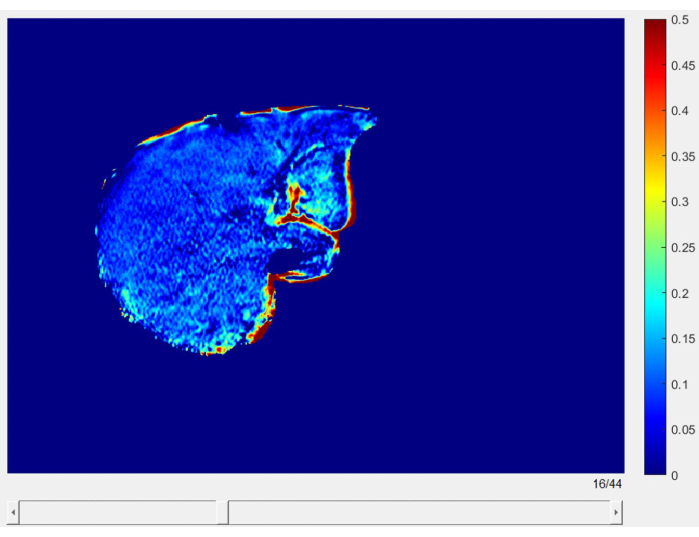
Figure 5: Liver fat fraction slices. High-resolution slices displaying the liver fat fraction map, providing a detailed view of LFF distribution throughout the entire liver. Please click here to view a larger version of this figure.
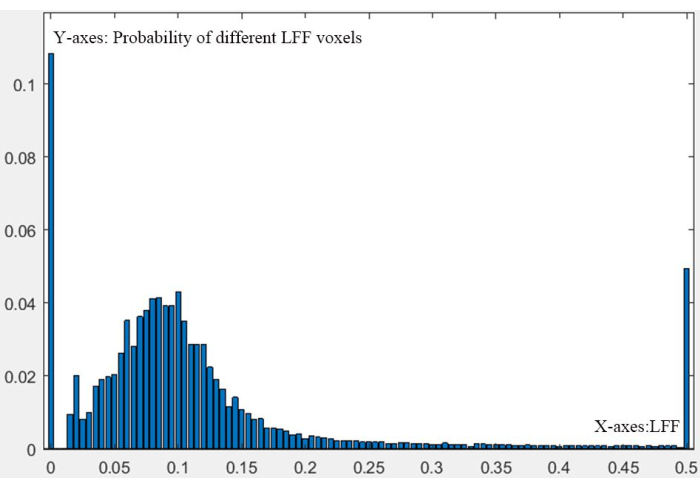
Figure 6: Whole liver 3D-LFF distribution. A figure depicting the numeric probability distribution of liver fat fraction (LFF) across the entire liver, presented in a three-dimensional format. Please click here to view a larger version of this figure.
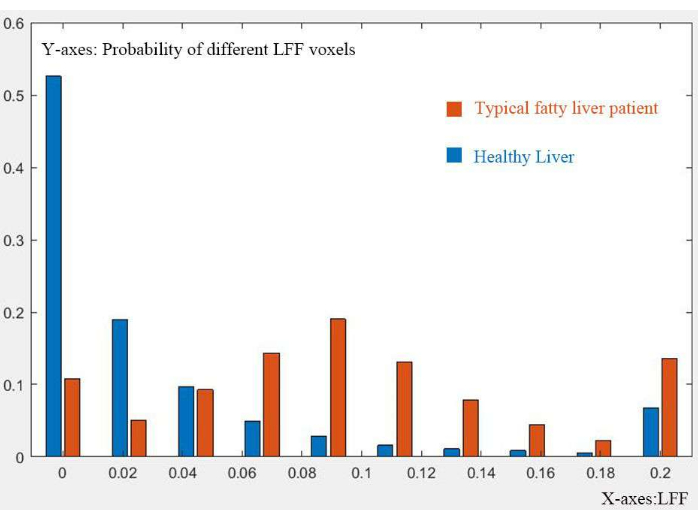
Figure 7: Comparison of 3D-LFF distribution. Comparison of the 3D-LFF distribution between a healthy liver and a typical fatty liver, highlighting differences in fat content and distribution. Please click here to view a larger version of this figure.
