The treatment procedure was approved by the institutional review board of The First Affiliated Hospital of Jinan University. Informed consent was obtained from the participant included in the study.
1. Patient selection for neoadjuvant therapy
- Inclusion criteria
- Select patients with lesions amenable to complete surgical removal (R0 resection).
- Select patients exhibiting high-risk factors for recurrence, including non-anatomical resection, vascular invasion, elevated serum AFP levels exceeding 32 ng/mL, tumor dimensions greater than 5 cm, presence of multiple tumors, and underlying cirrhosis.
- Exclusion criteria
- Exclude patients with high-risk recurrence factors who require surgical treatment at the time of initial diagnosis. Exclude patients unable to afford Y90 treatment.
2. Y-90 indications and dose evaluation
- DSA angiography for determining tumoral blood supply
- Ask the patient to lie supine for the procedure. Perform routine disinfection and draping. Apply a 4% lidocaine solution locally at the femoral artery puncture site for anesthesia.
- Adhere to routine handwashing procedures, don surgical attire, and wear sterile gloves.
- Insert a micropuncture needle into the right common femoral artery using the Seldinger technique. Follow this with the placement of a sheath connected to a saline flush system.
- Once the femoral artery puncture and catheter placement are successful (bright red arterial blood is observed), advance the angiographic catheter to the celiac trunk. If imaging suggests the presence of tumor-supplying vessels other than the hepatic artery, perform angiography on the superior mesenteric artery, the infra-diaphragmatic artery, etc., to identify any tumor-feeding vessels.
- Conduct angiography at the origin of the celiac trunk to determine if the hepatic tumor is exclusively supplied by a solitary branch of the right hepatic artery.
- Utilize the coaxial microcatheter technique for super selective catheterization on the right inferior branch of the right hepatic artery. Perform angiography to confirm the location of the supplying vessel.
- Technetium-99m (Tc-99m) MAA injection and imaging
- Inject 2 mCi of Tc-99m MAA through the microcatheter into the supplying arteries.
NOTE: This procedure is conducted in accordance with the Recommendations of the American Association of Physicists in Medicine on Dosimetry, Imaging, and Quality Assurance Procedures for 90Y Microsphere Brachytherapy in the Treatment of Hepatic Malignancies. The recommended dosage of Tc-99m MAA is set at 2-4 mCi (74-148 MBq)16. It's important to note that the dosage of Tc-99m MAA is fixed and does not vary based on the patient's weight, body surface area, or the size of the lesion. - Perform cone-beam computed tomography (CBCT) to delineate the targeted tumor region of intrahepatic Tc-99m MAA distribution. Manually outline the region on sagittal, coronal, and axial views during the arterial phase.
- Calculate the volume of the targeted tumor region using the SEG4 Properties option in CBCT.
- Inject 2 mCi of Tc-99m MAA through the microcatheter into the supplying arteries.
- LSF, TNR, and Y90 microsphere dosimetry calculations
- Configure the scan modes (SPECT and CT) parameters on the scanner and perform SPECT/CT imaging on the patient within 1-2 h post Tc-99m MAA infusion. Select the Fusion function to amalgamate the SPECT and CT images to determine the distribution of Tc-99m MAA in the liver, lung, and other organs.
- Calculate the lung shunt fraction (LSF) using planar imaging.
- Manually draw the regions of interest (ROIs), marking the distinct areas within the liver and lungs where the distribution of Tc-99m MAA is discernible in the anterior and posterior views of the liver, right lung, and left lung on the planar images. This step is performed by a nuclear medicine technologist.
NOTE: The Lung Shunt Fraction (LSF) represents the fraction of 99mTc-MAA that shunts from the liver to both lungs. Utilizing planar imaging, the nuclear medicine technologist manually draws ROIs around the liver and lungs (separately for the left and right lung) in both the anterior and posterior views. The counting result for each part is then obtained from this workstation. - Calculate the counts for each ROI using a standard nuclear medicine workstation. Use the formula:
Lung counts =

- Calculate the LSF using the equation:

- Manually draw the regions of interest (ROIs), marking the distinct areas within the liver and lungs where the distribution of Tc-99m MAA is discernible in the anterior and posterior views of the liver, right lung, and left lung on the planar images. This step is performed by a nuclear medicine technologist.
- Calculate the tumor-normal liver ratio (TNR) using three-dimensional (3D) segmentation application of SPECT/CT imaging.
- Manually draw discrete ROIs of the same size to encompass both tumor and normal liver areas based on the computerized tomography slices.
- Calculate the average count per unit cell of the tumor over the average count per unit cell of the normal liver in each ROI using a workstation.
- Calculate the TNR ratio using the following equation:

- Use the Partition model equation in the dose and activity visualizer for the Y-90 RE (DAVYR) application based on the results from the calculations to obtain the prescribed activity (Gbq) and dosage (Gy).
3. Y-90 TARE treatment
- Follow the approach described in step 2 and then perform an angiogram directly on the blood-supplying arteries identified in step 2.1.
- Compare the current angiographic image with that from step 2 to confirm the location of the supplying arteries more precisely.
- Advance the catheter to the supplying arteries after super selective catheterization, and then inject the Y90 microspheres, with the already calculated dose and activity, into the supplying arteries.
- For Y-90 TARE, obtain dedicated whole-body PET/CT scans from the chest to just above the pelvis. Perform PET-CT using the following parameters: 80 s to 110 s, 120 kVp, 40 mA, 1 s tube rotation, 4 mm slice collimation, and an 8 mm/s (i.e., pitch, 2) bed speed.
- Assess the TNR from a volume ROI drawn on the PET/CT images and then compare it with a TNR obtained from the SPECT/CT images of the Tc-99m MAA distribution to confirm the distribution of Y-90.
- When dispensing and injecting Tc-99m MAA and Y-90 microspheres, wear appropriate protective equipment, such as lead aprons, eye shields, and lead gloves.
- Do not perform any special treatment after Y-90 TARE treatment, and ask patients who have received Y-90 treatment to avoid close contact with others for 7 days to minimize the risk of radiation.
4. Sequential PD-1 inhibitor treatment after Y90 therapy
- Observe lesion stability for at least 2 months following Y90 treatment. Use appropriate imaging modalities for consistent monitoring. Re-evaluate the patient to determine the presence of any high-risk factors for recurrence.
- If high-risk factors are identified, evaluate patient suitability for immunotherapy, ensuring no contraindications are present. Select an appropriate PD-1 inhibitor, like Nivolumab or Pembrolizumab, based on the patient's financial considerations.
- Administer the chosen inhibitor in 1-2 cycles, each separated by 21 days. Administer the PD-1 inhibitor, prepared using 100 mL of physiological saline at 2 mg/mL, via peripheral intravenous injection over the course of 1 h, thereby completing one cycle of PD-1 inhibitor therapy.
- Post-treatment assessment and follow-up
- After completing PD-1 inhibitor therapy, follow-up imaging studies and tumor marker studies identical to those used pre-treatment.
- Assess the patient's monthly response to the PD-1 inhibitor therapy using standard evaluation criteria21.
5. Hepatectomy following Y90 TARE and PD-1 inhibitor
- Decision for hepatectomy: Assess the treatment site using the same radiological techniques previously applied to evaluate the stability of the lesion for a minimum of 2 months post PD-1 inhibitor therapy, ensuring no high-risk factors for recurrence are present.
- Preoperative preparations for hepatectomy: To accurately define tumor resection margins and inspect for possible metastatic lesions, administer Indocyanine green to the patient 3 days before surgery.
- Surgical procedure
- Perform tracheal intubation for general anesthesia on the patient positioned in a supine state. Carry out surgical disinfection for the upper abdominal region extending superiorly to the nipple line, inferiorly to the pubic symphysis, and laterally to the mid-axillary line.
- Upon entering the peritoneal cavity, use a laparoscope to conduct a thorough inspection of the liver and surrounding structures for any abnormalities or metastatic foci.
- Elevate the inferior border of the right liver with graspers to expose the tumor located in segment 6 (S6) of the liver.
- After injecting Indocyanine green intravenously, switch to fluorescence imaging mode to carefully assess the tumor's extent, ensuring no invasion into adjacent tissues or significant adhesions.
- Dissect the connective tissues between the inferior border of the right liver, posterior peritoneum, and right kidney using a harmonic scalpel. Progress superiorly dissecting the right triangular and coronary ligaments, thus exposing the second porta hepatis.
- Using duckbill forceps to retract the liver to the left to expose the right lobe fully.
- Employ fluorescence imaging mode to clearly delineate the margin between the tumor and adjacent healthy tissue.
- Mark the resection guide lines approximately 1-2 cm from the tumor margin using a monopolar cautery hook.
- Temporarily interrupt vascular inflow from the portal vein and hepatic artery to reduce intraoperative bleeding. Tighten the tourniquets in cycles of 15 min occlusion followed by 5 min reperfusion.
- Carefully transect the liver parenchyma along the guide lines with the harmonic scalpel. Coagulate small bile ducts and vessels with the scalpel, clamp first and then transect larger structures.
- After excising the tumor specimen, send it for histopathological evaluation.
- Rinse the hepatic cut surface with warm normal saline, followed by achieving hemostasis with bipolar coagulation. Use absorbable suture to close all incisions. The patient had a post-surgery hospital stay of 10 days. For post-surgical pain management, administer Tramadol via intramuscular injection.
- Follow-up post hepatectomy
- To promptly detect any potential postoperative recurrence or metastatic lesions, conduct follow-up examinations monthly for the first 3 months after surgery. Following this period, schedule examinations every 3 months for the next 2 years and then every 6 months for the subsequent 3 years, up to a total of 5 years post-surgery.
MRI revealed a reduction in liver volume, a wavy liver surface, and widened liver fissures of patients in this study. A nearly spherical mass, measuring approximately 7.2 cm x 5.6 cm x 6.6 cm, was identified in the right posterior lobe of the liver. The mass exhibited mixed low signals on T1-weighted imaging (T1WI), mixed high signals on T2-weighted imaging (T2WI), and high signals on diffusion-weighted imaging (DWI). It exhibited clear boundaries and heterogeneous arterial phase enhancement, suggesting the possibility of liver cirrhosis and HCC (Figure 1).
During catheter maneuvering, angiographic assessment was performed to confirm the absence of tumor-feeding vessels originating from the abdominal aorta, diaphragmatic arteries, and superior mesenteric artery. On angiography at the celiac trunk's origin, the segmental branch of the right hepatic artery (S6 or the right inferior branch) exhibited pronounced tortuosity and dilation. This observation established that the hepatic tumor received vascular supply exclusively from this singular arterial branch (Figure 2A). A foundational pre-assessment for Y-90 TARE involves mapping tests using Tc-99m MAA perfusion, exploiting the comparable dose distribution between Tc-99m MAA and Y-90 microspheres. Post-Tc-99m MAA injection, the perfusion zone for Tc-99m MAA was delineated, with the calculated perfusion volume for the target tumor being 246.27 mL (Figure 2A). Patients demonstrating an LSF greater than 20% are at an increased risk for radiation-induced lung damage, rendering them typically unsuitable candidates for Y-90 treatment22. A heightened TNR signifies a more potent tumoricidal effect while adhering to the maximal permissible liver radiation dose. The calculated LSF stood at 17.17%, and the TNR was registered at 8.2 (Figure 2B).
The partition model, in comparison to the Medical Internal Radiation Dose (MIRD) and Body Surface Area (BSA) methods, provides superior personalized radiation dose estimation by factoring in the TNR, enhancing individualized treatment planning. Results from the partition model indicate radiation doses of 36.6 Gy for the normal liver (below the 40 Gy threshold), 17.6 Gy for the lung tissue (within the 20 Gy limit), and a peak dose of 300 Gy for the tumor, necessitating a Y-90 microsphere activity of 1.36 GBq (Figure 3A). Post Y-90 TARE therapy (Figure 3B), a PET/CT scan was performed, indicating no off-target spread or coverage discrepancies (Figure 3C).
At 1 month after the Y-90 TARE treatment, the tumor was reduced to 6 cm, and the AFP level decreased to 21,155 ng/mL. At 3 months post-treatment, the tumor showed no significant changes. Given the persistent high risk of recurrence, treatment with a PD-1 inhibitor was initiated. At 5 months following Y-90 TARE therapy (2 months after starting PD-1 inhibitor treatment), the lesion had further reduced to 4 cm, and the AFP level had dramatically decreased to 1.84 ng/mL (Figure 4 and Table 1).
Images of the tumor during hepatectomy under both white light and fluorescence are presented (Figure 5A). The tumor specimens which were obtained from hepatectomy were transformed into frozen sections for gross pathology. When examined microscopically, they revealed no tumor cells, deposition of Y-90 microspheres, significant lymphocytic infiltration, and cirrhotic changes in the adjacent normal liver tissue23 (Figure 5B). At 12 months post-operation, follow-up, and assessment for recurrence were conducted, with MRI imaging indicating no evidence of recurrence or metastasis (Figure 5C).
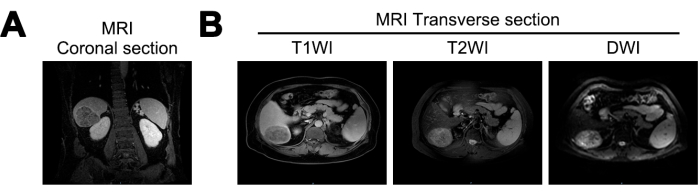
Figure 1: Magnetic-Resonance Imaging (MRI) imaging at initial diagnosis. (A) Coronal section of MRI T1 Weighted Imaging (T1WI) signal, (B) transverse sections of MRI T1WI, T2 Weighted Imaging (T2WI), and Diffusion Weighted Imaging (DWI) signals. Please click here to view a larger version of this figure.
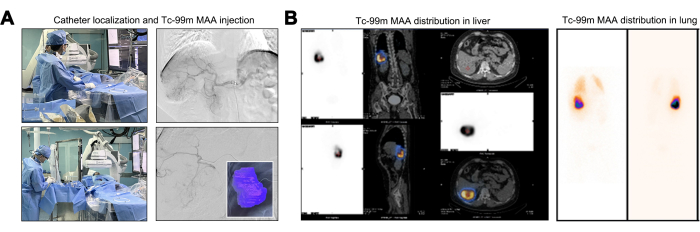
Figure 2: Injection and distribution of Technetium-99m Macroaggregated Albumin (Tc-99m MAA). (A) Illustration of the injection process of Technetium-99m macroaggregated albumin (Tc-99m MAA). (B) Presentation of the dose distribution of 99mTc MAA in the liver. Please click here to view a larger version of this figure.
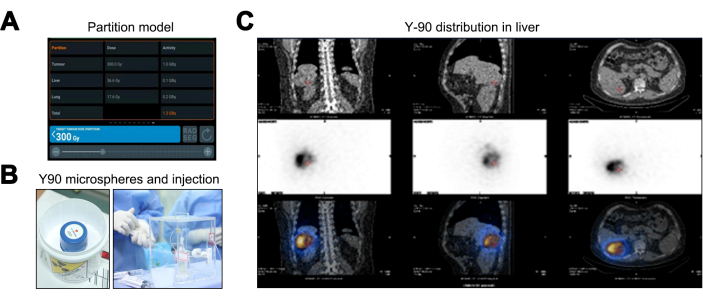
Figure 3: Yttrium-90 Transarterial Radioembolization (Y-90 TARE) treatment process. (A) Depiction of the data calculated using the Partition model. (B) The packaging and injection of the Y-90 microspheres. (C) Single-photon Emission Computed Tomography/Computed Tomography (SPECT/CT) to validate the dosage distribution of the Y-90 microspheres. Please click here to view a larger version of this figure.
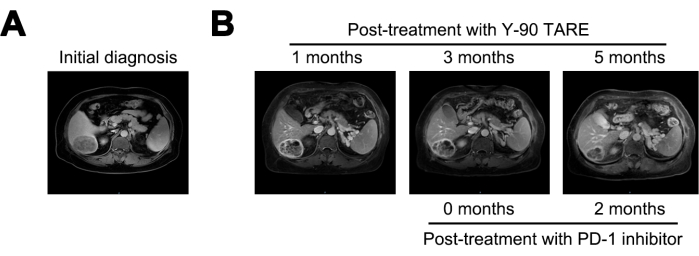
Figure 4: Tumor comparison. (A) Presentation of the MRI image at initial diagnosis, while (B) displays the MRI images at 1-, 3-, and 5-months post-treatment with Y-90 TARE. Programmed Cell Death-1(PD-1) inhibitor treatment was performed 3 months after Y-90 TARE. The patient underwent treatment with a PD-1 inhibitor 3 months after the Y-90 TARE procedure. Please click here to view a larger version of this figure.
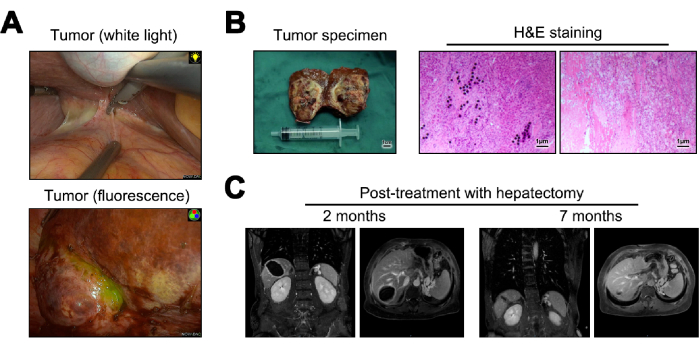
Figure 5: Hepatectomy and subsequent follow-up. (A) Presentation of the tumor observed intraoperatively. (B) Illustration of the postoperative tumor specimen and Hematoxylin and Eosin (H&E) staining. (C) MRI images at 2- and 12-months post-surgery. Please click here to view a larger version of this figure.
| Post-treatment with Y-90 TARE | |||||
| Initial diagnosis | 1 months | 3 months | 5 months | ||
| AFP (ng/mL) | 66840 | 21155 | 19535 | 1.84 | |
Table 1: Post-treatment AFP level measurement.
