When the protocol is executed successfully, 1 g of pancreas tissue yields approximately 100-200 slices. Subsequently, these slices should undergo stereomicroscope inspection to identify those rich in islets before proceeding with functional assessments. Viability, determined by labeling with Fluorescein Diacetate (FDA) and Propidium Iodide (PI), is expected to reach 80%-90% (Figure 2A). Viability may be notably lower at the cutting surface due to cell damage during the slicing process. In viable slices, dynamic hormone secretion (Figure 2B) is observed, resulting in robust insulin release upon exposure to high glucose and membrane depolarization with Potassium chloride (KCl).
Conversely, when there are delays during the slicing procedure or the tissue quality is suboptimal, the outcomes differ significantly. The number of obtained slices may decrease, and the viability assessment may indicate a higher proportion of non-viable cells labeled with PI (Figure 2C). In these cases, the functional assessment indicates a diminished or even absent response to high glucose and membrane depolarization (Figure 2D). The data from suboptimal experiments illustrate the importance of precise execution in a timely manner and tissue quality, as they can lead to reduced tissue viability and impaired functionality. These negative outcomes serve as a valuable reminder of the critical factors to consider in the success of this method.
Common findings in calcium imaging are visualized as a heat map, as depicted in Figure 5D, or as separate traces for individual cells, as presented in Figure 5E. It is important to emphasize that the dye labels all cell types indiscriminately, hence specific stimuli are essential for distinguishing cells based on their responses. To identify viable cells, we employ KCl and sort the cells based on responses that exceed the average baseline response by more than two standard errors. Moreover, slices can be fixed and stained, enabling identification of cell types.
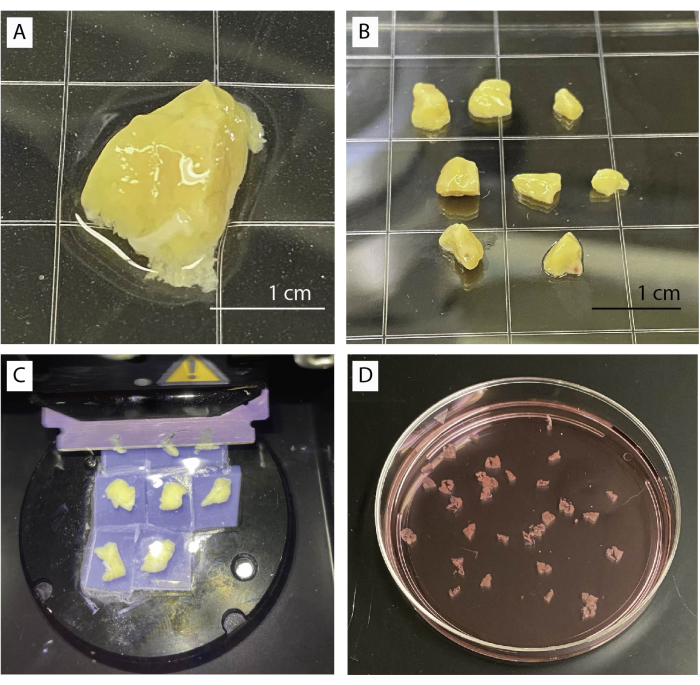
Figure 1: Tissue processing and slicing. (A) 1 g of unprocessed pancreas tissue. (B) Cleaned pancreas pieces ready for agarose embedding. (C) Slicing procedure using a vibratome. (D) Freshly cut human pancreas slices. Please click here to view a larger version of this figure.
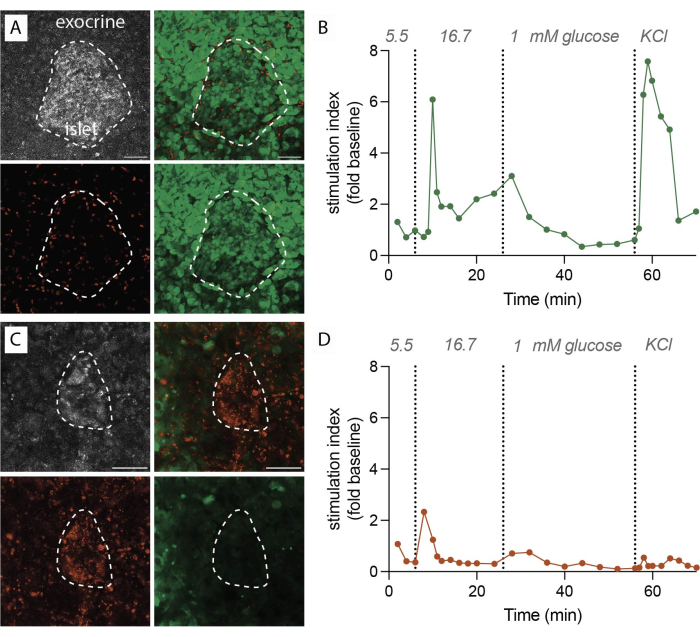
Figure 2: Tissue viability and insulin secretion data. (A) Representative images for viable tissue slices. Maximum intensity projection of reflected laser light (grey, top left), PI for dead cells (red, bottom left), FDA for living cells (green, bottom right), and merged images for live and dead cells (top right). Dotted line indicates an islet. Scale bar 50 µm. (B) Dynamic insulin secretion of human pancreatic tissue slices from a single nondiabetic donor. The insulin kinetics show a first phase peak response after 6 min of high glucose stimulation, followed by a plateau second phase. Data is normalized to the average baseline secretion at 5.5 mM glucose (stimulation index, fold change). Secretion has been performed on slices from the same donor as shown in (A). (C) Representative images for non-viable tissue slices. Maximum intensity projection of reflected laser light (grey, top left), PI for dead cells (red, bottom left), FDA for living cells (green, bottom right), and merged images for live and dead cells (top right). Dotted line indicates an islet. Scale bar 50 µm. (D) Dynamic insulin secretion of human pancreatic tissue slices from a single nondiabetic donor. The insulin kinetics demonstrate a clear loss of both glucose stimulated insulin secretion and membrane depolarization with KCl. Data is normalized to the average baseline secretion at 5.5 mM glucose (stimulation index, fold change). Secretion has been performed on slices from the same donor as shown in (C). Please click here to view a larger version of this figure.
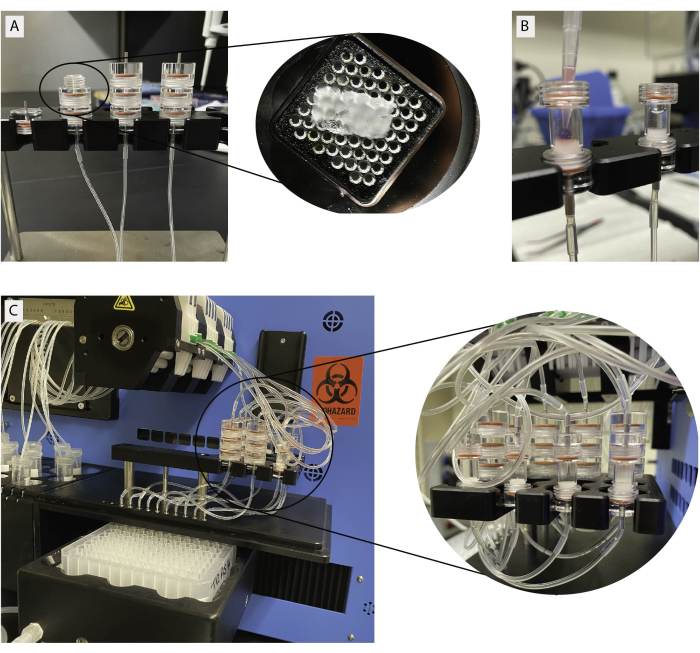
Figure 3: Tissue loading for dynamic perifusion. (A) Stacked slice chambers. Individual slices are loaded on a metal grid as shown in the insert. (B) Loading of isolated islets in islet chambers. Slice and islet chambers connected to perifusion machine. Please click here to view a larger version of this figure.
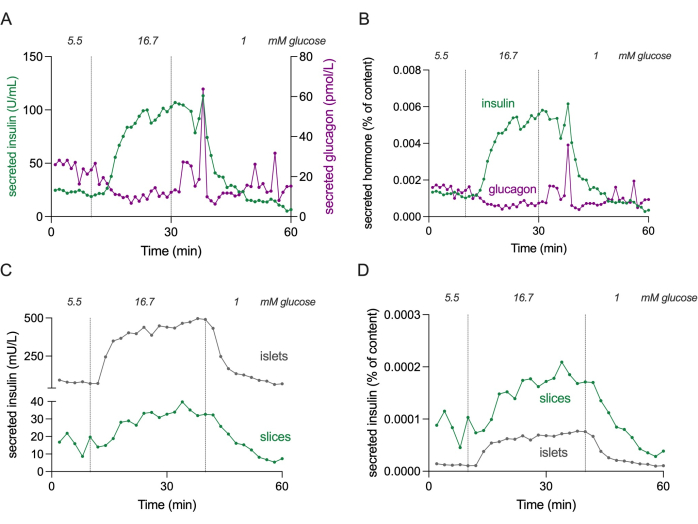
Figure 4: Hormone secretion in slices and isolated islets. Data shown in panels (A) and (B) originate from a different donor compared to panels (C) and (D). (A) Absolute hormone secretion from 3 pancreatic tissue slices from a single nondiabetic donor. Insulin secretion is shown in green and glucagon secretion in magenta. (B) Hormone secretion shown in (A) normalized to total hormone content (% of content). Content is measured from all 3 slices used in the experiment. (C) Dynamic insulin secretion of isolated islets (100 islets) and pancreatic tissue slices (3 slices) from the same nondiabetic donor. Data is shown in absolute numbers (mU/L). (D) Insulin secretion shown in (C) normalized to total insulin content (% of content). Please click here to view a larger version of this figure.
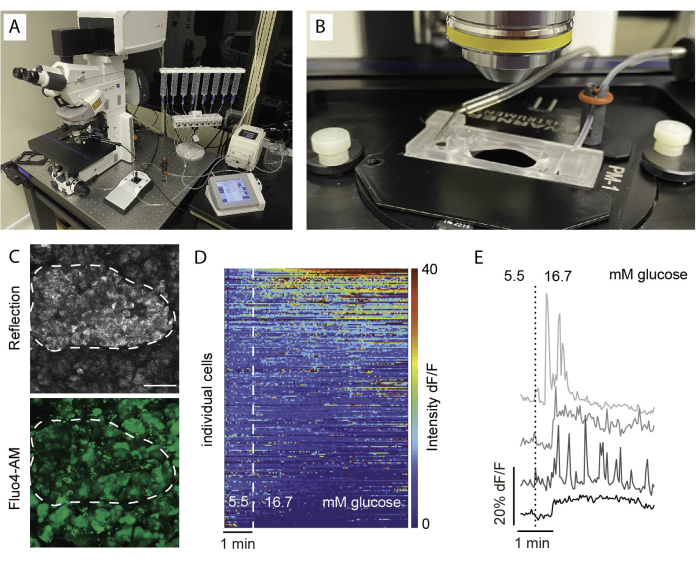
Figure 5: Imaging setup and expected results. (A) Setup for functional imaging with an upright confocal microscope and a perifusion setup. (B) Imaging chamber connected to inflow and outflow. (C) Z stack of confocal images of an islet within a tissue slice from a healthy human donor showing reflected light (top) and Fluo4 signal (bottom). Reflection is used to identify islets within the slice (dotted line). (D) Heatmap showing in vitro Ca2+ dynamics of islet cells expressed as the fluorescent intensity of Fluo4 normalized to the basal signal intensity at 5.5 mM glucose and stimulation with high glucose (16.7 mM). Each row represents a single cell followed over time in the x-axis and their response in magnitude change (%) of the fluorescent intensity over baseline (dF/F) shown in the color scale from blue (low intensity) to red (high intensity). (E) Representative traces of 4 individual cells showing a response to high glucose. Please click here to view a larger version of this figure.
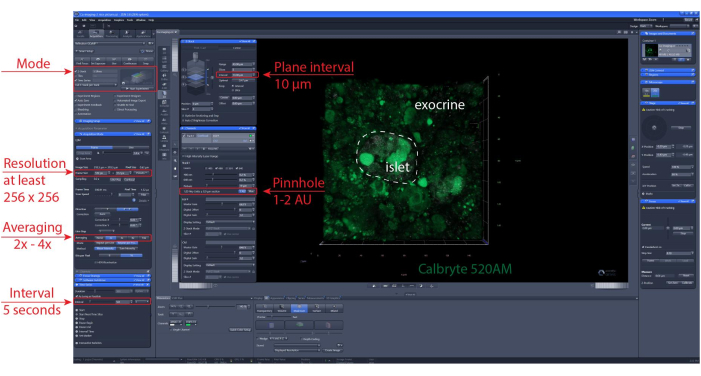
Figure 6: Calcium imaging settings. Screenshot of the software of representative settings chosen to perform time-lapse recordings of 40 µm (XYZT imaging). Please click here to view a larger version of this figure.
