Surgical phase
It is important to mention that both animal models used in this study present certain constraints due to the induced diseases. These constraints regarding the manipulation of hard and soft tissues are reflected during the surgical procedure.
In the diabetic model, the rat is larger, making it difficult to stabilize the legs during surgical procedures. This increases the surgical time and, consequently, the anesthesia time, which requires a longer recovery time and, therefore, requires greater vigilance in the postoperative period.
As for the osteoporotic model, the requirements were very different, being more concentrated at the time of bone manipulation. In this case, it is possible to observe greater bleeding during the drilling procedure. In addition, the implant placement process becomes more difficult. Some complications may occur, such as small cracks in the bone, altering the progression of the implant during its entry and making it more unstable due to the lack of bone resistance on the lateral walls of the implant. This limitation requires more manual pressure and stabilization during placement, making it more difficult to control until the correct positioning of the implant is achieved.
Regarding the maximum implant insertion torque, relatively different values were observed for the two diseases (Table 1). In general, the maximum average insertion torque observed for the osteoporotic model was higher than for the diabetic model. With these results, it is interesting to understand the effect that diabetes has on bone density and bone resistance to implant insertion, as this condition appears to have a more severe effect on the mechanical properties of bone compared to osteoporosis.
Postsurgical analysis
The adequate placement of the titanium implants after 4 weeks and 12 weeks of implantation was analyzed by micro-CT imaging. Representative images are provided for both osteoporotic (Figure 9) and diabetic (Figure 10) rats. Overall, the implants were correctly implanted through the cortical and trabecular tibiae, showing intimate and continuous contact with the cortical part, and without any signs of inflammation or adverse reactions, thus proving the success of the surgical protocol for both models of pathology.
Collectively, the analysis of the images also allowed for calculating the ratio of bone area (mm2) versus implant area (mm2), referred to as V(BIC), at the cortical region, and comparing the performance of the surgical procedure over time and within models. As shown in Figure 11, V(BIC) values remained constant for the osteoporotic model at 4 weeks and 12 weeks, indicating a stable integration of the implant over time and highlighting that an intimate connection with bone is ensured already at 4 weeks. Of note, very similar values were obtained for the diabetic model, thus showing the adequacy of the study protocol for both models of pathology.

Figure 1: Surgical field. The surgical field showing the correct position of the rat and exposure of the area to be intervened, adaptation of the conical adaptor to the airways for maintenance of the anesthesia during the procedure, as well as the instruments necessary for the intervention. Please click here to view a larger version of this figure.

Figure 2: Surgical incision. Correct stabilization of the rat's paw and, at the same time, fixing the thin mobile skin to obtain a correct incision. Please click here to view a larger version of this figure.
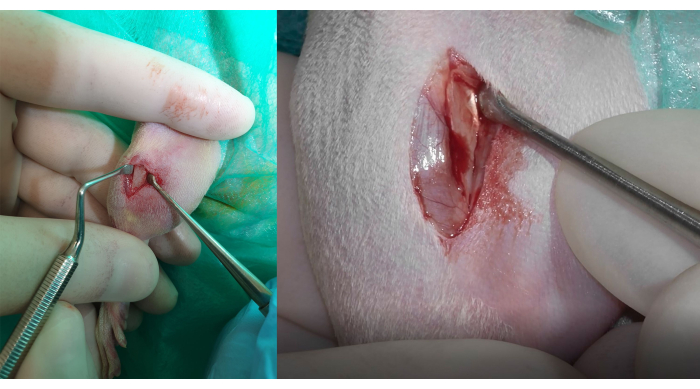
Figure 3: Bone exposure and muscle insertion Identification. Left side: total detachment of the tissues with the consequent bone exposure. To preserve and avoid damage to the insertion of the tibialis cranialis muscle, the gracilis, and the gastrocnemius lateral head muscles, it is important to correctly identify the fibrous white tissue firmly adhered to the bone, visible in the figure on the right side. Please click here to view a larger version of this figure.

Figure 4: Drilling sequence. The drilling process sequence begins with the lance pilot drill on the left, followed by the twist drill on the right. To ensure a stable and safe drilling procedure, it is important to maintain both leg and soft tissue stabilization during drilling. Please click here to view a larger version of this figure.

Figure 5: Preparation for implant insertion. The implant is inserted on an intermediate piece to be submitted to the cleaning process with a saline solution while the implant rotates at 20 rpm. This intermediate piece allows the insertion of the implant into the bone with an electronic device. This device ensures control of the implant insertion speed and records the real-time insertion torque. Please click here to view a larger version of this figure.

Figure 6: Titanium implant placement. Placing the implant within the bone requires its placement on the flat face of the medial bone, away from the proximal border of the anterior-medial face of the bone. Please click here to view a larger version of this figure.
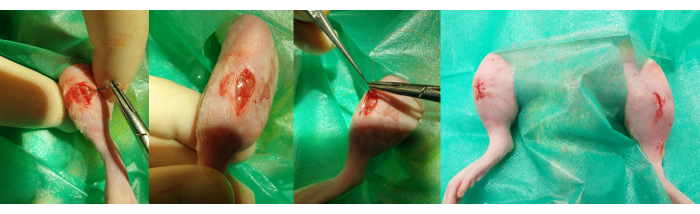
Figure 7: Wound closure. The steps for closing the wound are observed in 2 different planes. Left: the first, deeper plane is made with simple stitches to approximate the edges of the muscle tissue. Right: the second, more superficial plane is carried out with an intradermal suture to approximate the skin while preventing the knot from being in an externalized position. Please click here to view a larger version of this figure.
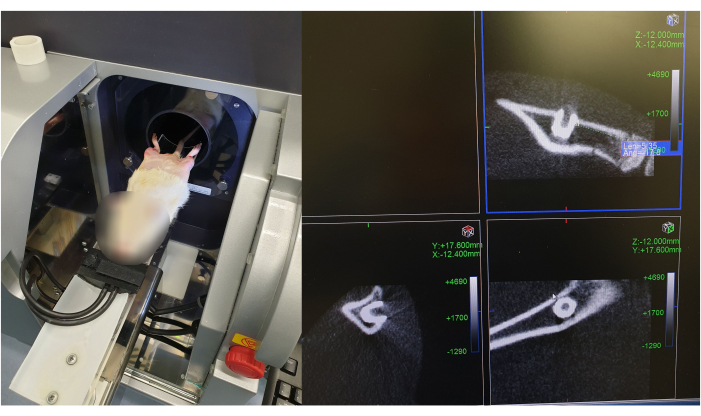
Figure 8: Micro-CT scan of implant placement after surgical procedure. The figure illustrates the positioning of the rat in the Micro-CT scanner, and the images of the implant position are divided into three sections, corresponding to the x-, y-, and z-views, respectively. The implant is pointed with a red arrow in the different views. Please click here to view a larger version of this figure.

Figure 9: Micro-CT scan of an implant placed in the tibia of an osteoporotic rat. Representative postsurgical micro-CT images of titanium implants placed in the tibiae of osteoporotic rats after (A) 4 weeks and (B) 12 weeks of implantation. Each image is divided into three sections, corresponding to the x-, y- and z-views, respectively. Please click here to view a larger version of this figure.
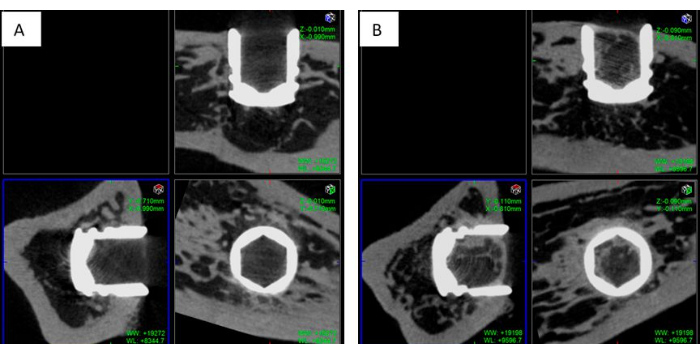
Figure 10: Micro-CT Scan of an implant placed in the tibia of a diabetic rat. Representative postsurgical micro-CT images of titanium implants placed in the tibiae of osteoporotic rats after (A) 4 weeks and (B) 12 weeks of implantation. Each image is divided into three sections, corresponding to the x-, y- and z-views, respectively. Please click here to view a larger version of this figure.

Figure 11: Bone-implant contact (BIC) analysis. V(BIC) values calculated as bone area (mm2) *100/ implant area (mm2) from micro-CT images for the osteoporotic (Osteo) and diabetic (Diab) models after 4 weeks (4 w) and 12 weeks (12 w) post-implantation. Please click here to view a larger version of this figure.
| Maximum implant insertion torque [N·cm] | ||
| Model | Right leg | Left leg |
| Osteoporosis | 6.11 ± 0.96 | 6.49 ± 1.34 |
| Diabetes | 4.79 ± 1.70 | 4.90 ± 1.76 |
Table 1: Maximum insertion torque. Differences in maximum torque values obtained during implant insertion between diabetic rats and osteoporotic rats. Diabetic rats present lower maximum torque values than osteoporotic rats.
