This study was approved by the Human Research Ethics Committee of Edith Cowan University, Reference Number REMS 2021-02489-STEINWANDEL. Informed consent was obtained from workshop participants, and a copy of a participant information sheet was provided. Only workshop participants who participated in one of the ultrasound workshops during the delivery period between the years 2021 and 2022 were invited to participate and included in this study. All subsequent workshop participants in 2023 and 2024 were excluded from participation in this study.
1. Creation and preparation of the simulation model12
- Cut a regular raw chicken breast with a sharp kitchen knife horizontally to allow for the insertion of three or more fluid-filled artificial blood vessels, which will simulate human blood vessels in this experiment.
- Preparation of the artificial blood vessels
- Fill modeling balloons (size 260Q) with cold rosehip tea or water prepared with red food color using a 50 mL catheter-tipped syringe. Fill the modeling balloon with the prepared fluid and remove any surplus air from the balloon.
- Push the fluid in the balloon and remove any air bubbles at the same time by repeatedly pushing the syringe in and out of the modeling balloon. When this repetitive process is completed, the balloon must be free of air bubbles and slightly pressurized.
- Tighten the modeling balloon with a knot to avoid any fluid leaks.
- Place the fluid-filled modeling balloon on the lower half of the chicken breast. Fold the other chicken breast half over (placed) on top. Wrap this chicken breast simulation model with a transparent film and place it on a tray (Figure 1).

Figure 1: Simulation model. The simulation model was created from raw chicken breast and fluid-filled modeling balloons (260Q). Please click here to view a larger version of this figure.
2. Simulated vascular access cannulation
- Place a charged POCUS device (portable or stationary) with a linear probe and a probe cover onto this simulation model of patient tissue prepared in step 1.
- Apply some ultrasound gel to the area of interest in the simulation model. Don a pair of non-sterile gloves.
3. Measurement of the depth and caliper of a vessel
- In a transverse view of the simulated blood vessel in the simulation model, visualize a simulated vessel and achieve a good vision of the vessel of interest by placing the ultrasound probe on top of the simulation model and centering the view of the vessel in the middle of the screen of the ultrasound device, where it will appear as a black circular structure. Ensure a reasonable size of the vessel can be identified, taking up at least 1/3rd of the screen.
- Place this vessel in the center of the screen of the POCUS device by moving the ultrasound probe across the simulation model so that the whole vascular structure is visible. Adjust image size and contrast settings on the ultrasound device, if required, to obtain optimal vision of the vessel and surrounding tissue, to distinguish between vessel space and surrounding tissue. Freeze the image by pressing the Freeze function button on the ultrasound device.
- On the frozen image, place digital markers, to indicate the depth of the center of the vessel. Place digital markers as well to measure the diameter (caliper) of the vessel (Figure 2).
NOTE: This information helps the observer make critical decisions on the size and length of cannula needed, which may be suitable for potentially reaching this particular blood vessel and enabling successful cannulation.

Figure 2: Vessel measurement. Measurement of the simulated vessel (transverse view) on the ultrasound screen. Please click here to view a larger version of this figure.
4. Observation of the direction of the vessel
- Rotate the ultrasound probe by 90° to obtain a longitudinal view of the blood vessel. This view allows the observer to make a decision on the direction of the vessel and the intended cannulation, providing crucial information prior to the subsequent process of the actual cannulation.
- Observe the direction of the vessel being aligned with the ultrasound probe. Once the vessel direction has been observed, use this to decide which direction of cannula placement might likely be useful and also successful for the insertion and placement of the cannula, even when the vessel might appear to be at a deeper level and may not be palpable or visible from the outside (Figure 3).

Figure 3: Longitudinal view of a simulated vessel. Please click here to view a larger version of this figure.
5. Cannulation of a deep vessel
NOTE: Combining all this information, a virtual picture of that vessel is created in the observer's mind; the process of vascular cannulation will follow.
- Place the linear probe in a transverse view of the vessel. Remove the protective needle cover of the PIVC cannula to commence the cannulation procedure.
- Place the transverse vision of the vessel centrally on the screen of the POCUS device. Slowly and carefully cannulate (perpendicular) in the middle of the linear probe the simulation model at an angle of around 40° and aim for the top (upper end) of the vessel.
- Advance the needle tip into the tissue of the simulation model and aim for the vessel. Try to identify visually the needle tip on the screen of the POCUS device while it is advanced through the tissue by simultaneously advancing the needle but also following the needle tip with the ultrasound probe (Figure 4).
- Final placement of the cannula with the use of POCUS
- Further advance the needle through the tissue towards the vessel and follow slowly with the ultrasound probe, the needle tip simultaneously in the same motion as the needle advancement.
NOTE: Through this the clinician can ensure that the needle tip is always visible in the desired anatomical space within the simulation model tissue and then moving towards the intravascular space. - Visualize the needle tip entering the intravascular space, then level the needle to a shallower angle and further advance the needle to finally rest it in the center of the vessel of the simulation model (final destination).
- Validate the position of the needle tip with the POCUS device by observing the needle tip on the screen by changing the angle of the ultrasound probe or moving the ultrasound in small (mm) increments back and forth until the needle tip visually disappears/reappears on the screen.
- Observe the opposite end of the PIVC for some evidence of red-colored fluid to confirm correct placement. Remove the stylet from the PIVC (Video 1).
- Further advance the needle through the tissue towards the vessel and follow slowly with the ultrasound probe, the needle tip simultaneously in the same motion as the needle advancement.

Figure 4: Transverse view of a simulated vessel. Please click here to view a larger version of this figure.
Video 1: Cannula advancement into the center of the vessel. Please click here to download this Video.
A total of 81 individuals participated in 11 half-day workshops between 2021 and 2022. Most participants were resident medical officers (n=43, 53%), followed by staff development/clinical nurses and clinical nurse consultants (n=19, 25.3%) with a mean of 8 years of clinical experience. Half of the participants (n=40, 49%) had only 2 years or less of clinical experience. There were also some other workshop participants, such as a nuclear medicine technologist, a dental sedationist, and a diagnostic radiologist. Almost a quarter of all participants were employed at satellite hemodialysis (HD) clinics. Ultrasound devices were available in almost all workplaces (n=75, 92.6%). Most participants (n=55,67.9%) were female and had a mean age of 35.7 years (Table 1).
Workshop participants followed the instructions of the workshop facilitator and were able, after some theoretical instructions and observing the facilitator demonstrating the task in a simulation model, to successfully perform the same cannulation process using a POCUS device in connection with the described simulation model step-by-step.
Workshop participants were invited to complete an electronic survey prior to and directly at the conclusion of the workshop, indicating their level of confidence in using POCUS for USGPIVC. These surveys consisted of 11 closed and three open-ended questions, and participants were able to rate their individual skills using ultrasound while cannulating on a 10-point rating scale, ranging from 0=not very skilled to 10= very proficient. Eight weeks after conclusion of the workshop, participants were again invited to complete a final survey to indicate any progress of their current skill in adopting and using the newly learned skill in their clinical practice. In this last survey, nine closed and two open-ended questions regarding their self-assessed USGPIVC skill were asked. Data analysis was done using SPSS statistics. The individually self-assessed cannulation skill using POCUS resulting from three different electronic surveys at three-time points were analyzed, and a Friedman Test and post hoc analysis were conducted using the Wilcoxon sign-ranked tests with a Bonferroni correction applied. A p-value < 0.05 was considered statistically significant, and content analysis was conducted on the responses to the open-ended questions (Figure 5, Table 2).
The self-evaluated cannulation skill exhibited a statistically meaningful variation across the three time periods (p < 0.001). Post hoc analysis unveiled a statistical distinction in self-assessed cannulation proficiency prior to the workshop when contrasted with the period immediately following the workshop (p < 0.001) and 8 weeks after the workshop (p < 0.001). However, no significant differences in self-evaluated cannulation skills using POCUS were observed between the immediate post-workshop period and the 8-week follow-up (p=.722). Some workshop participants reported on the conclusion of the workshop that at their workplace, management allows the use of ultrasound only before cannulations to help the clinician visualize vessels and to give the operator a better impression and understanding of specific individual vascular conditions before any cannulation attempt has been made.
Most workshop participants claimed that attending the workshop using simulation models had enhanced their clinical skill in using ultrasound for the purpose of cannulating a venous vessel significantly and that they gained more confidence in using this technique at the conclusion of the workshop, which further advanced after applying this technique in their clinical environment. At 8 weeks after the conclusion of the workshop, participants were again invited to complete another electronic version of the survey. Most participants were able to practice this newly learned skill subsequently in their clinical environment with patients, and as in most of their clinical institutions, POCUS devices were available (Table 3; Table 4).
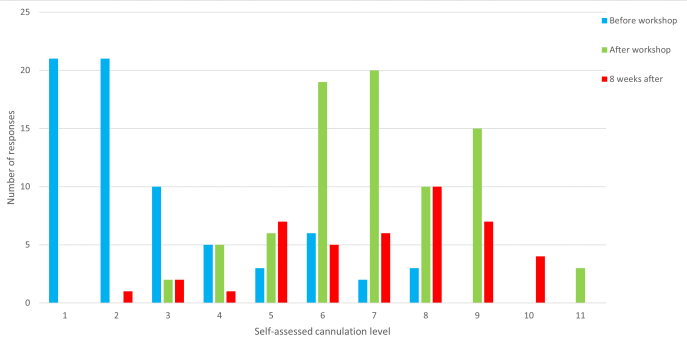
Figure 5: Self-assessment of cannulation skills. Level of self-assessed cannulation skill level provided by participants before, directly after (on conclusion) and 8 weeks after the workshop. Prior to the workshop, the Median was 1, IQR: 0 to 3; After the workshop, the Median was 6, IQR: 5 to 7; 8 weeks later, the Median: 6, IQR: 4 to 8. The n number is 81 before the workshop, 80 after the workshop, and 43 for 8 weeks after. This figure has been modified from8. Please click here to view a larger version of this figure.
Table 1: Baseline demographics. This table has been modified from8. Please click here to download this Table.
Table 2: Self-assessment of cannulation skills. The p-values of self-assessed cannulation skills by participants before, directly after, and 8 weeks after the workshop The n number is 81 before the workshop, 80 after the workshop, and 43 for 8 weeks after. This figure has been modified from8. Please click here to download this Table.
Table 3: Post-workshop evaluation. This table has been modified from8. Please click here to download this Table.
Table 4: Evaluation at 8 weeks after workshop completion. This figure has been modified from8. Please click here to download this Table.
