Rotating the Intraocular Lens to Prevent Posterior Capsular Opacification in Cataract Surgeries
Summary
The present protocol describes removing residual epithelial cells by rotating the intraocular lens in extracapsular cataract surgery without extra tools for preventing posterior capsular opacification.
Abstract
Posterior capsule opacification (PCO) is a common postoperative complication of extracapsular cataract surgery, which is caused by the proliferation and migration of lens epithelial cells and can affect long-term visual outcomes significantly. The most effective treatment for PCO is neodymium-doped yttrium aluminum garnet (Nd:YAG) laser capsulotomy; however, this treatment is associated with posterior segment complication and can break the stability of capsular bag, affecting the position and function of trifocal or toric intraocular lenses (IOLs). Advances in surgical procedures, IOL design, and pharmacy have reduced the rate of PCO in recent years, concentrating on the inhibition of proliferative lens epithelial cells (LECs). This protocol aimed to clear LECs more thoroughly during phacoemulsification and IOL implantation. The first several steps, including clear corneal incision, continuous circular capsulorhexis, hydrodissection, hydrodelineation, and phacoemulsification, were completed as conventional procedures. After placing the IOL into the capsular bag, rotation of the IOL by at least 360° was performed using an irrigation/aspiration tip or a hook, with slight stress on the posterior capsule. Some residuals occurred in the originally transparent capsular bag after rotation of the IOLs. Then, these materials and the viscoelastic were cleared completely using an irrigation/aspiration system. A clear posterior capsule was observed after the surgery in patients undergoing this method. This method of rotating IOLs is a simple, effective, and safe way to prevent PCO by clearing residual LECs and can be carried out without extra tools or skills.
Introduction
Cataracts are the most common cause of blindness worldwide, characterized by a clouding of the lens. The only means of treating cataracts is surgical intervention by removing the opaque lens, which restores high visual quality. However, a secondary reduction of visual quality, termed posterior capsule opacification (PCO), develops in 20%-40% of patients within 2 to 5 years after surgery1. This article introduces a method to further remove residual lens epithelial cells (LECs) left in the capsular bag in cataract surgery by rotating the intraocular lens (IOL) to prevent PCO.
PCO is a process caused by LECs, which are inevitably left in the capsular bag following cataract surgery and then begin to proliferate and migrate2. During phacoemulsification, a capsular bag is generated by continuous curvilinear capsulorhexis in the anterior capsule, which comprises a part of the anterior capsule, the equatorial capsule, and the entire posterior capsule2,3. In most patients, an IOL is implanted into the capsular bag. A transparent capsular bag, especially the posterior capsule, permits the light to transmit into the eyes, which is necessary for good postoperative visual quality4. A proportion of LECs are usually still attached to the capsular bag. As a reaction to the surgical trauma and a foreign body response toward IOLs, the residual epithelial cells start to proliferate and occupy first the remaining part of the anterior capsule, and then all available surfaces, including the surface of IOL and, most importantly, the previously acellular posterior capsule4. Subsequently, cells continue to divide, ultimately covering the entire posterior capsule and affecting the visual axis. The following changes, including fibrosis and regenerative form5, can cause significant visual impairment6.
PCO that affects visual acuity can be treated with capsulotomy of the posterior capsule, usually by a neodymium-doped yttrium aluminum garnet (Nd:YAG) laser and sometimes a surgical procedure4. Recent studies report that the incidence of Nd:YAG capsulotomy for treating PCO 3 years after surgery is between 5% and 20%7,8. However, this procedure can break the normal posterior capsular morphology and wrinkle the posterior capsule, thus likely affecting the position of IOLs, which is unfavorable to the long-term visual outcome of IOLs, especially multifocal IOLs, and toric IOLs6. Advances in surgical procedures, IOL design, the pharmacological inhibition of LEC proliferation, and the induction of LEC apoptosis have been confirmed useful in preventing PCO, most of which target the LECs9.
LECs are normally distributed over the inner side of the anterior lens capsule in single-layer form1. LECs distributed in the area around the equatorial lens are the natural site of division, which is known as the germinative zone, while the dividing cells are also observed on the anterior capsule10,11. It has also been shown that equatorial cells can proliferate and migrate in the posterior capsule12. Residual LECs in the capsular bag are responsible for PCO. If LECs in the germinative zone are cleared as much as possible during cataract surgery, the possibility of PCO occurring postoperatively decreases as a consequence. As far as it is known, routine phacoemulsification does not include a procedure to remove equatorial LECs. In a study in India, the author proposed that rotation of the IOL by a Sinskey hook13 in the capsular bag decreases PCO and Nd:YAG capsulotomy rate.
Here, we introduced a method by rotating the IOL using an irrigation/aspiration (I/A) tip in the capsular bag to prevent PCO in cataract surgeries. The rationale of this method relies on the mechanical contact between the IOL and the capsular bag, especially the equatorial area, to remove residual LECs. Compared with treating PCO using Nd:YAG capsulotomy, the prevention of PCO maintains the integrity of the posterior capsule and the correct position of IOLs. Additionally, this method is cost-effective and requires no extra tools, which applies to cataract phacoemulsification and IOL implantation. Different from anterior capsule polishing, which is conducted using an I/A tip in the polishing mode of the phaco system6,14, the rotation of the IOL is conducted after the IOL implantation and is supposed to further remove visible lens matter (cortex) and cells.
Protocol
This study adhered to the tenets of the Declaration of Helsinki. The study protocol was approved by the Institutional Review Board of Peking University Third Hospital. It should be noted that the novel procedure here is the step of rotating the IOL. The inclusion criteria are cataract patients over 50 years of age willing to undergo cataract surgery in Peking University Third Hospital. The exclusion criteria are the presence of eye diseases that may affect the stability of the suspensorium and capsular bag, such as pathologic myopia, glaucoma, pseudoexfoliation syndrome, uveitis, subluxation of the lens including Marfan syndrome, Marchesani syndrome, and homocystinuria.
1. Surgery preparation
- Patient preparation
- Use 0.5% levofloxacin eye drops four times per day 3 days before surgery. Administer topical anesthetic eye drops of 0.4% oxybuprocaine hydrochloride three times per 5 min before the surgery (see Table of Materials).
NOTE: Patients' pupils become dilated with compound tropicamide eye drops (0.5% tropicamide and 0.5% phenylephrine hydrochloride) 1 h before surgery.
- Use 0.5% levofloxacin eye drops four times per day 3 days before surgery. Administer topical anesthetic eye drops of 0.4% oxybuprocaine hydrochloride three times per 5 min before the surgery (see Table of Materials).
- Equipment settings
- Ensure the following settings for the phacoemulsification device system (see Table of Materials): 30%-95% torsional nucleus chop, 90 cm bottle height, 260-450 mm Hg vacuum, and 36 cc/min aspiration flow rate.
2. Rotating using the irrigation and aspiration (I/A) system
- Corneal incision
- Make a 3.2 mm limbal incision at the steepest meridian using a 3.2 mm slit blade (see Table of Materials). A "Z"-shaped multiplanar corneal incision is preferred. First, create a 0.3 mm deep groove perpendicular to the corneal surface and insert the blade into the groove with its tip tangentially directed to the corneal surface, thereby creating a tunnel through the clear cornea into the anterior chamber.
- Create a 0.8 mm subsidiary incision 90° anti-clockwise using a 20 G side port microvitreoretinal (MVR) knife (see Table of Materials).
- Phacoemulsification
- Open the capsule with a continuous curvilinear capsulorhexis using Utrata capsulorhexis forceps (see Table of Materials) under viscoelastic conditions.
- Perform cortical-cleaving hydrodissection by placing a blunt-tipped cannula with balanced salt solution (BSS) under the anterior capsule flap, carefully lifting the capsular, and injecting BSS in a radial direction, to separate the cortex from the posterior capsule.
- Perform hydrodelineation by injecting BSS into the substance of the nucleus to separate the harder nucleus from the peripheral softer nucleus.
- Under the mode of "chop", bury the phaco tip into the center of the nucleus and insert the phaco tip (see Table of Materials) under the anterior capsule flap, cracking the nucleus into two pieces using Sinskey hook (see Table of Materials). Repeat this step to create multiple small wedges of the nucleus for phacoemulsification.
- Irrigation and Aspiration (I/A)
- Modulate the machine in "cortex" mode. Use the I/A tip (see Table of Materials) to accomplish cortical cleanup. Remove the soft epinucleus and peripheral cortical material.
- IOL insertion
- Fill the capsule bag and anterior chamber with viscoelastics (see Table of Materials). Load a foldable single-piece IOL (see Table of Materials) into an injector cartridge prefilled with viscoelastic.
- Introduce the tip of the injector through the incision and insert the IOL by pushing the tail of the injector, with the anterior haptic spreading into the capsular bag. Place the posterior haptic under the anterior capsule using the tip of the injector.
- Rotating the IOL and removing the viscoelastic
- Use the I/A tip to remove the viscoelastic from the anterior chamber. During this procedure, rotate the IOL clockwise at least 360° using the I/A tip with slight posterior pressure.
- Aspirate the residual fragments and viscoelastic in the capsular bag by inserting the I/A tip behind the optic part of the IOL.
3. Rotating using IOL hooks
- The steps before insertion of the IOL are the same as the first four steps (2.1-2.4) above. In this method, after the IOL is inserted into the capsular bag, use a Fenzl hook (see Table of Materials) to rotate the IOL clockwise at least 360° and slide the IOL in the capsular bag from side to side, putting slight pressure on the posterior capsule at the same time.
4. Follow-up procedures
- Instill BSS from the paracentesis incision using a blunt-tipped cannula to reform the anterior chamber.
- Inject BSS into both sides of the corneal tunnel incision. If the incision leaks, the wound should be sutured with a 10-0 nylon suture.
Representative Results
A clear capsular bag was formed after the I/A step (Figure 1A). However, some cortical fragments were observed in the capsular bag after rotating and polishing the IOL (Figure 1B).
This process can also be performed using a hook. Similarly, the posterior capsule was clear after capsular polishing by the I/A tip (Figure 2A). Through fast rotation and movement of the IOL, some residuals appeared in the capsular bag behind the IOL (Figure 2B).
IOL movement in the capsule has two functions. On the one hand, this procedure achieves adequate contact between the haptics and the equator of the lens capsule. Under the tangential force of the I/A tip, the IOL can rotate in the capsular bag to allow haptics to disrupt epithelial cells within the equatorial region to remove the cells and reduce the formation of PCO. On the other hand, the sliding of IOLs makes the optical part of the IOL come into contact with the posterior capsule. The I/A tip or hook puts the IOL slide in the capsule bag from side to side, polishing the posterior capsule.
We collected 20 eyes that had undergone cataract surgery (10 eyes with rotation of IOL and 10 eyes without rotation). Follow-ups were conducted at 1 day, 1 week, and 3 months postoperatively, and the existence of PCO was evaluated each time. The demographic data and PCO results of patients are shown in Table 1. Figure 3 is a retro illumination image showing an example of PCO, and a clear and transparent capsular bag is shown in Figure 4.
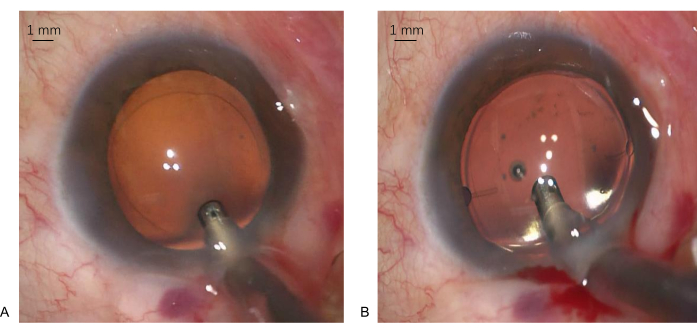
Figure 1: Capsular bag appearances during surgery using an I/A tip. (A) The posterior capsule is very clean after conventional polishing by the I/A instrument. (B) After rotation of IOL by the I/A tip, there are fragments in front of the posterior capsule. Magnification: 10x. Scale bars: 1 mm. Please click here to view a larger version of this figure.
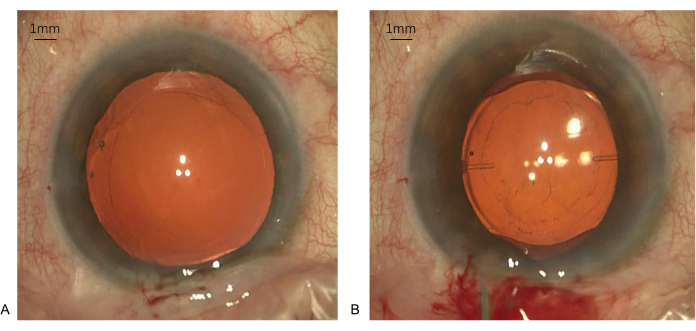
Figure 2: Capsular bag appearances during surgery using a Fenzl hook. (A) The posterior capsule is quite clear after polishing by the I/A instrument. (B) After the rotation of the IOL by a hook, some residuals appeared in the capsular bag behind the IOL. Magnification: 10x. Scale bars: 1 mm. Please click here to view a larger version of this figure.
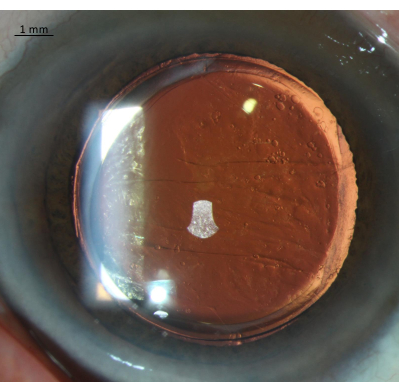
Figure 3: The image of PCO via retro illumination. This is an example of a patient with PCO. Magnification: 20x. Scale bar: 1 mm. Please click here to view a larger version of this figure.
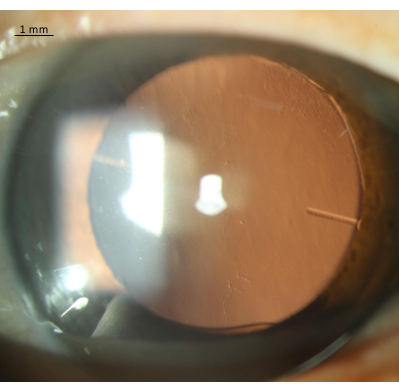
Figure 4: Image of the posterior capsule 1 year post-operatively. After 1 year, the capsular bag was still clear and transparent. Magnification: 20x. Scale bar: 1 mm. Please click here to view a larger version of this figure.
| Age (year-old) | Gender (female: male) | Number of patients with PCO | ||
| Rotation group (n = 10) | 71.3 ± 7.7 | 04:06 | 1 | |
| Non-rotation group (n = 10) | 70.3 ± 7.5 | 05:05 | 3 | |
Table 1: Demographic data and PCO results of the patients. PCO: posterior capsular opacification.
Discussion
There are some benefits to this method. Firstly, residual LECs in the capsule bag were reduced further, especially those in the equatorial area, and the possibility of PCO occurrence was reduced rationally. Secondly, a reduced possibility of PCO means a lower rate of Nd:YAG laser treatment, providing the opportunity to maintain the integrity of the capsule bag and effective lens positions and functions. Thirdly, this method can be achieved with available instruments in cataract surgery without additional preparation. In order to achieve the purpose of preventing PCO, it is necessary to understand its biological process first. Anterior LECs surrounding the rhexis have the characteristic of in situ growth, and seem more likely to express α smooth muscle actin and become myofibroblasts, causing opacity and wrinkling of the anterior capsule15,16. Equatorial LECs (LECs-E) maintain the characteristics of stem cells, with the ability of active division and migration, and are more likely to form Elschnig's pearls16. Vision is lost when PCO on the center of the visual axis affects light scattering into the eyes. Therefore, the measures to prevent PCO aim at clearing LECs-E and preventing their proliferation and migration to the posterior capsule. This method fundamentally minimized the possibility of residual LEC, which is the first step in preventing PCO.
A number of studies have proposed different approaches for attempting the prevention of PCO, including pharmacological inhibition of cell proliferation, induction of LEC apoptosis, improvement of IOL design, and surgical skills, but none have succeeded in preventing PCO completely1,17,18,19,20. Apple et al. identified six factors influencing PCO: hydrodissection-enhanced cortical cleanup, in-the-bag fixation of IOLs, moderate-sized anterior capsulorhexis diameter, highly biocompatible IOL material, maximal contact of the IOL optic and posterior capsule, and IOL optical geometry with square, truncated edges9. All these factors mainly target the removal of residual LECs and cortex or maintaining appropriate IOL position in the capsular bag to form a barrier preventing cell migration. Advances in IOL engineering have contributed to the prevention of PCO. Previous studies have found that eyes with AcrySof IOLs, which is a polyacrylic lens, are associated with a reduced degree of PCO and lower YAG rates21,22. However, in a classical study, Nishi et al. demonstrated that the beneficial effect of AcrySof IOLs on PCO prevalence was mainly due to its square edge profile23. The square edge prevents the LECs from migrating onto the posterior capsule by putting higher pressure on it by forming a physical barrier15. The results of a meta-analysis have supported this theory, revealing that a major factor preventing PCO is the design of sharp-edged IOLs24, which are associated with less PCO formation and a lower Nd:YAG capsulotomy rate than round-edged IOLs during the observation period25. Different from previous trials, Joshi et al. proposed that the rotation of hydrophilic, dual-haptic IOLs in the capsular bag by a Sinskey hook decreases PCO and the Nd:YAG capsulotomy rate, while there still remains a low rate of PCO and laser treatment13.
This study aimed at cleaning residual LECs in the capsular bag by rotating IOLs using an I/A tip or a hook, which provided more chances of mechanically removing LECs, especially equatorial cells. In eyes implanted with haptic plate IOLs, there was a larger area of contact between the IOL and capsular bag, and a sharp-edged IOL design made the contact more total and effective26. In addition, previous studies have shown that plate-haptic IOLs have greater rotational stability than loop haptics27,28. It remains unknown what is the best way to target LECs for PCO prevention, and it seems that a specific way is insufficient. Improving surgical equipment, like femtosecond laser technology, to complete precise capsulorhexis and remove cataracts through very small incisions may contribute to PCO rates29.
The critical points in this method include: (1) the inclusion criteria should be strict; only patients with normal zonula and an intact capsular bag are considered. (2) One-piece IOLs designed with haptics should be chosen, particularly plate haptic IOLs, which provide a more accessible surface with the capsular bag, especially the equatorial part. (3) The I/A needle should be operated at the iris plane, moving the IOL with tangential force. Too much downward pressure should be avoided. In this article, the author introduced two ways to rotate the IOL, and this procedure can be modified by using any other tool to rotate. There are some limitations to this method. Firstly, it may have higher requirements for the surgical skills of surgeons. Secondly, large-sample, well-designed, large-scale comparative studies on different IOL designs should be performed for reliable results. Thirdly, an in vitro experimental study in animal or donor eyes is needed to validate whether rotation of the IOL affects equatorial cells or not.
In summary, the advantage of this method for preventing PCO is that it requires no additional materials or tools and can be achieved easily through only one step in cataract surgery. This method is cost-effective and applicable in surgeries of cataract phacoemulsification and IOL implantation.
Disclosures
The authors have nothing to disclose.
Acknowledgements
This article is funded by Beijing Haidian Innovation and Transformation Project, HDCXZHKC2021212.
Materials
| 20 G Sideport MVR Knife | BVI | 378231 | To make corneal incision |
| 3.2 mm Slit Blade | BVI | 378232 | To make corneal incision |
| Balanced salt solution | Xingqi | H19991142 | Compound electrolyte intraocular irrigating solution |
| Centurion vision system | Alcon Laboratories | 8065753057 | The Centurion Vision System is indicated for emulsification, separation, irrigation, and aspiration of cataracts, residual cortical material and lens epithelial cells, vitreous aspiration and cutting associated with anterior vitrectomy, bipolar coagulation, and intraocular lens injection. |
| Compound tropicamide eye drops | Xingqi | Zhuobian | To dilate the pupils before the surgery |
| Disposable sterile irrigator | WEGO | 100038404339 | To complete hydrodissection and hydrodelineation |
| Fenzl lens insertion hook and manipulator | Belleif | IF-8100 | IOL positioning hook |
| Levofloxacin eye drops | Santen | Cravit | To prevent ocular infection before the surgery |
| Mini-flared Kelman tip 30DG | Alcon Laboratories | 8065750852 | To complete phacoemulsification |
| One piece intraocular Lens | Zeiss | AT TORBI 709M | Intraocular lens |
| Oxybuprocaine hydrochloride | Santen | Benoxil | Topical anesthesia |
| Phaco handpiece | Alcon Laboratories | 8065751761 | To complete phacoemulsification |
| Sinskey hook | Belleif | IF-8013 | For chop |
| Ultraflow II I/A tip | Alcon Laboratories | 8065751795 | To complete irrigation and aspiration |
| Utrata capsulorhexis forceps | Belleif | IF-3003C | To complete continuous circular capsulorhexis |
| Viscoelastics/Medical sodium hyaluronate gel | Bausch&lomb | iviz | Maintaining the anterior chamber and capsular bag |
References
- Nibourg, L. M., et al. Prevention of posterior capsular opacification. Experimental Eye Research. 136, 100-115 (2015).
- Wormstone, I. M., Eldred, J. A. Experimental models for posterior capsule opacification research. Experimental Eye Research. 142, 2-12 (2016).
- Sela, T. C., Hadayer, A. Continuous curvilinear capsulorhexis – a practical review. Seminars in Ophthalmology. 37 (5), 583-592 (2022).
- Wormstone, I. M., Wormstone, Y. M., Smith, A. J. O., Eldred, J. A. Posterior capsule opacification: What’s in the bag. Progress in Retinal and Eye Research. 82, 100905 (2021).
- Wu, W., et al. The importance of the epithelial fibre cell interface to lens regeneration in an in vivo rat model and in a human bag-in-the-lens (BiL) sample. Experimental Eye Research. 213, 108808 (2021).
- Darian-Smith, E., Safran, S. G., Coroneo, M. T. Lens epithelial cell removal in routine phacoemulsification: is it worth the bother. American Journal of Ophthalmology. 239, 1-10 (2022).
- Leydolt, C., et al. Posterior capsule opacification with two hydrophobic acrylic intraocular lenses: 3-year results of a randomized trial. American Journal of Ophthalmology. 217, 224-231 (2020).
- Ursell, P. G., Dhariwal, M., O’Boyle, D., Khan, J., Venerus, A. 5 year incidence of YAG capsulotomy and PCO after cataract surgery with single-piece monofocal intraocular lenses: a real-world evidence study of 20,763 eyes. Eye. 34 (5), 960-968 (2020).
- Apple, D. J., et al. Eradication of posterior capsule opacification: documentation of a marked decrease in Nd:YAG laser posterior capsulotomy rates noted in an analysis of 5416 pseudophakic human eyes obtained postmortem. Ophthalmology. 108 (3), 505-518 (2020).
- Wormstone, I. M., et al. Human lens epithelial cell proliferation in a protein-free medium. Investigative Ophthalmology & Visual Science. 38 (2), 396-404 (1997).
- Fisus, A. D., Findl, O. Capsular fibrosis: a review of prevention methods and management. Eye. 34 (2), 256-262 (2020).
- Eldred, J. A., Zheng, J., Chen, S., Wormstone, I. M. An in vitro human lens capsular bag model adopting a graded culture regime to assess putative impact of IOLs on PCO formation. Investigative Ophthalmology & Visual Science. 60 (1), 113-122 (2019).
- Joshi, R. S., Chavan, S. A. Rotation versus non-rotation of intraocular lens for prevention of posterior capsular opacification. Indian Journal of Ophthalmology. 67 (9), 1428-1432 (2019).
- Liu, X., Cheng, B., Zheng, D., Liu, Y., Liu, Y. Role of anterior capsule polishing in residual lens epithelial cell proliferation. Journal of Cataract and Refractive Surgery. 36 (2), 208-214 (2010).
- Boyce, J. F., Bhermi, G. S., Spalton, D. J., El-Osta, A. R. Mathematical modeling of the forces between an intraocular lens and the capsule. Journal of Cataract and Refractive Surgery. 28 (10), 1853-1859 (2002).
- Spalton, D. Posterior capsule opacification: have we made a difference. The British Journal of Ophthalmology. 97 (1), 1-2 (2013).
- Wang, R., et al. Surface modification of intraocular lens with hydrophilic poly(sulfobetaine methacrylate) brush for posterior capsular opacification prevention. Journal of Ocular Pharmacology and Therapeutics. 37 (3), 172-180 (2021).
- Liu, S., Zhao, X., Tang, J., Han, Y., Lin, Q. Drug-eluting hydrophilic coating modification of intraocular lens via facile dopamine self-polymerization for posterior capsular opacification prevention. ACS Biomaterials Science & Engineering. 7 (3), 1065-1073 (2021).
- Sureshkumar, J., Haripriya, A., Muthukkaruppan, V., Kaufman, P. L., Tian, B. Cytoskeletal drugs prevent posterior capsular opacification in human lens capsule in vitro. Graefes Archive for Clinical and Experimental Ophthalmology. 250 (4), 507-514 (2012).
- Eid, A. M., Abd-Elhamid Mehany Elwan, S., Sabry, A. M., Moharram, H. M., Bakhsh, A. M. Novel technique of pneumatic posterior capsulorhexis for treatment and prevention of posterior capsular opacification. Journal of Ophthalmology. 2019, 3174709 (2019).
- Hollick, E. J., et al. The effect of polymethylmethacrylate, silicone, and polyacrylic intraocular lenses on posterior capsular opacification 3 years after cataract surgery. Ophthalmology. 106 (1), 49-54 (1999).
- Ursell, P. G., et al. Relationship between intraocular lens biomaterials and posterior capsule opacification. Journal of Cataract and Refractive Surgery. 24 (3), 352-360 (1998).
- Nishi, O., Nishi, K., Wickstrom, K. Preventing lens epithelial cell migration using intraocular lenses with sharp rectangular edges. Journal of Cataract and Refractive Surgery. 26 (10), 1543-1549 (2000).
- Li, N., et al. Effect of AcrySof versus silicone or polymethyl methacrylate intraocular lens on posterior capsule opacification. Ophthalmology. 115 (5), 830-838 (2008).
- Maedel, S., Evans, J. R., Harrer-Seely, A., Findl, O. Intraocular lens optic edge design for the prevention of posterior capsule opacification after cataract surgery. The Cochrane Database of Systematic Reviews. 8 (8), (2021).
- Schartmuller, D., et al. Posterior capsule opacification and Nd:YAG laser rates with two hydrophobic acrylic single-piece IOLs. Eye. 34 (5), 857-863 (2020).
- Patel, C. K., Ormonde, S., Rosen, P. H., Bron, A. J. Postoperative intraocular lens rotation: a randomized comparison of plate and loop haptic implants. Ophthalmology. 106 (11), 2190-2195 (1999).
- Zhu, X., Meng, J., He, W., Rong, X., Lu, Y. Comparison of the rotational stability between plate-haptic toric and C-loop haptic toric IOLs in myopic eyes. Journal of Cataract and Refractive Surgery. 46 (10), 1353-1359 (2020).
- Tassignon, M. J. Elimination of posterior capsule opacification. Ophthalmology. 127, S27-S28 (2020).
