1. Intubation
- Equipment needed for endotracheal intubation: means of assisted ventilation, slings for opening the mouth, low pressure suction with blunt tip, veterinary laryngoscope with straight blade between 17 and 25 cm long, stylet, syringe with air, stethoscope and adhesive tape. For adult Göttingen minipigs an endotracheal tube size 5 to 7 mm is appropriate10. In this video a 5.5 mm tube was used 10.
- The minipig is placed on its back and properly supported in order to ensure that the laryngeal passage is kept straight.
- The tongue is pulled out slightly and the jaw held open by an assistant without overextending the head. Rotation of the airways or excessive extension of the head can occlude airways, making the laryngeal opening more difficult to identify and complicating tracheal placement of the tube.
- The laryngoscope is passed into the pharyngeal cavity and used to depress the tongue, making the epiglottis visible. The tip of the suction is used to displace the epiglottis from the soft palate. The tip of the laryngoscope is then used to press the epiglottis upward toward the base of the tongue, revealing the laryngeal opening.
- The arytenoids cartilages and vocal cords come into view and the endotracheal tube is advanced gently with a slight rotation, into the trachea during expiration.
- The tube cuff is inflated according to the specifications of the manufacture while taking care to avoid excess inflation, which may cause swelling and edema of the airways. Pigs have a bronchus to ventilate the right cranial pulmonal lobe. It is therefore important to place the tube above the tracheal bifurcation. This is facilitated by using the correct tube size and importantly by fastening the proximal end of the tube at the level of the snout using adhesive tape.
- When the minipig is properly intubated, a free passage of air must be felt through the tube, and chest auscultation should reveal respiration sounds in both the left and right side of the thorax.
- Upon connecting the ventilator with monitoring system to the minipig, physiological expiratory carbon dioxide values should be measurable and the carbon dioxide curve that follows the respiration pattern decided by the ventilator settings6,10 can be observed.
- The carbon dioxide and oximetry values may initially be affected by the premedication and anesthesia induction. However these values should quickly revert back to normal with proper ventilation6,10. Any sign of cyanosis despite artificial-assisted ventilation indicate improper placement of the tube. The most common error is inadvertent placement of the tube in the esophagus.
2. Transurethral bladder catheterization
- This procedure is only for female pigs. For adult minipigs a Foley catheter French size 8 or 10 is appropriate. Due to the curvature and size of the external urethral opening, a catheter with stylet is preferable. A nasal speculum can be used in small minipigs whereas a speculum with longer blades can be useful for large animals. Necessary equipment also includes a blunt-tip forceps, a syringe with saline, lubricant and a closed system urine drainage bag.
- In order to best visualize the external urethral orifice during catheterization the minipig is placed on its back with a support under the lumbar region, while an assistant pulls the hind legs cranially.
- The lubricated speculum is inserted and opened to visualize the vaginal wall. The female external urethral opening is located in the floor of the vagina approximately one-third to one-half of the distance to the cervix (Fig. 1A). However, because the animal is placed on the back, the position of the urethral opening will appear to be inverted.
- The catheter is controlled with the blunt-tip forceps, so the tip of the catheter is in continuation of the forceps. Carefully insert the catheter in the urethral opening (Fig. 1B). The urethra is easily traumatized if too much force is used during catheterization. However, slight resistance may initially be felt until the catheter has passed the external urinary sphincter. If this problem persists, this may indicate that the animal is not sedated deeply enough. The solution is to wait awhile and let the anesthesia take its effect.
- As the catheter reaches the bladder, remove the stylet, and urine will be seen flowing.
- Inflate the balloon with saline according to the specifications of the manufacture and gently pull the catheter out until the balloon catches on the bladder neck.
- Attach the closed-system urine drainage bag.
- Tape the catheter to the tail to avoid accidental displacement of the catheter when handling the animal.
3. Femoral artery and vein catheterization
- Necessary equipment includes: scalpel, blunt-tip surgical scissors, tissue forceps, small blunt-tip surgical forceps, small self-retaining tissue retractor, needle holder, surgical swaps, suture with needle, heparinized saline as a flush-fluid to maintain catheter patency, two 18-gauge IV cannula, two 4-French brite tip sheaths with introducer and Seldinger guide wire.
- The depth of anesthesia should be assessed by testing the interdigital pain reflex before initiating the procedure.
- The femoral artery and vein are approached with the minipig placed on its back and the rear leg retracted laterally. Identify in the skin fold between the gracilis and sartorius muscle where the pulsation of the superficial part of the medial saphenous artery disappears.
- Make a longitudinal superficial skin incision cranial to this point, thereby avoiding inadvertently damaging the medial saphenous vessels.
- Use a blunt-tip scissors to dissect the underlying subcutaneous tissue.
- The fascia division of the sartorius and gracilis muscle is divided cranial to the penetration site of the medial saphenous vessels, first with a small blunt-tip surgical forceps and then digitally.
- The two muscle groups are separated with a small self-retaining tissue retractor while taking care not to damage the femoral nerve and vessels.
- The artery is isolated for a length of approximately 1 to 2 cm using blunt dissection.
- Rotate the beveled venflon needle so the lumen is facing upwards. Bend the needle a little so it will follow the vessel curvature more easily. Remember to ensure the needle still can move back and forth with little effort.
- The artery is punctured, the needle retracted and the Seldinger guide wire is inserted through the venflon tube.
- Remove the venflon tube while gently applying pressure on the artery to ensure fixation of the guidewire.
- The sheath with introducer is inserted over the Seldinger wire and advanced to the desired position, after which the introducer and Seldinger wire is removed.
- The femoral vein is located just below and medial to the artery. After isolating the vein using blunt dissection, the vein is cannulated as previously described for the artery.
- To verify that both the artery and vein are correctly catheterized, draw blood from both sheaths and compare the color of the samples. Whenever drawing a blood sample, remember to subsequently flush the catheters with heparinized saline in order to maintain catheter patency.
- The catheters are secured and the skin is closed with a few sutures.
- A vessel loop can be placed around the artery and vein in order to fixate the vessels prior to puncture. Despite its advantages, we generally avoid this additional step, because it requires excess dissection of the vessels and can increase the risk of damaging the lateral and deep branches.
4. Transcardial perfusion
- The following equipment is needed for the procedure: perfusion system (Fig. 2), relevant perfusion fluids, scalpel, blunt-tip surgical scissors, bone shears, and two large self-holding forceps of which at least one has a curved tip. A self retaining sternal retractor is not absolutely necessary, but it eases the procedure considerably.
- Transcardial perfusion must be performed in a well ventilated room with a high power fume extraction system and facilities that allow collection of perfusate liquids and blood for subsequent safe disposal.
- After intravenously injecting a lethal dose of pentobarbital, test the interdigital pain reflex before continuing.
- The best access to the heart and aorta is provided via a median sternotomy. Make a deep longitudinal skin incision, extending from the manubrium to the xiphoid process of the sternum. Gain access to the thoracic cavity by making a small incision in the diaphragm just below the xiphoid process.
- Insert the bone shears into the thoracic cavity and bisect the sternum. Care must be taken when performing this procedure, because the heart may be adherent at some place to the inside of the sternum. Therefore, make certain that the blade of the bone shears rests at all time inside the thoracic cavity against the inside of the sternum.
- After the sternum has been divided, put in the self-retaining sternal retractor and open the thoracic cavity.
- If still intact, make a small incision in the pericardium at the apex of the heart and then digitally open the pericardial sac.
- Identify the left ventricle, the right auricle and the aorta together with the superior caval vein (Fig. 1C)
- Make a small superficial cut near the apex of the heart and access the left ventricle by perforating the myocardium with a blunt-tipped instrument.
- Insert the perfusion cannula inside the left ventricle and move the cannula tip cranially into the aorta.
- When the cannula is felt between the fingers in the aorta, clamp the cannula into place with the self-holding curved forceps.
- Make an incision in the right auricle and begin injecting the fixative through the perfusion cannula. The flow of perfusate in the aorta can be felt, and blood will pour out through the incised right auricle as the perfusate flow into the minipig vessels continues. Notice how systemic perfusion with paraformaldehyde induces hyperextension of the limbs and twitching of the superficial musculature due to aldehyde cross-linkage of nerves and muscles. When using a perfusion system powered by compressed air instead of gravity, make sure to remove the cannula, or clamp the clear silicone tube, before the canister is empty, in order to avoid air from entering the vascular system.
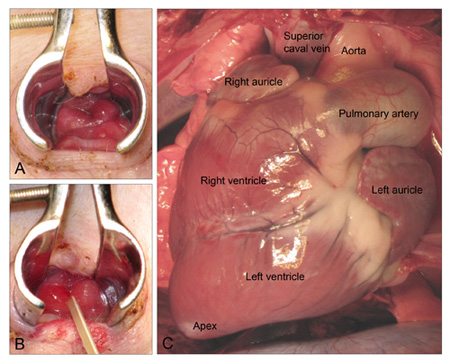
Figure 1. A: The female Göttingen minipig external urethral opening. B: The urethral opening after insertion of catheter. C: Ventral view of the minipig heart after median sternotomy.
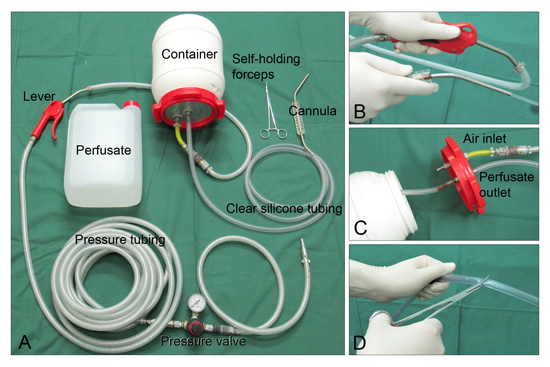
Figure 2. A: The perfusion system consists of inlet tubing with an adjustable pressure valve and a lever used to control inlet of compressed air into the container holding the perfusate. Clear silicone tubing connects the container to a blunt-tip cannula made from a 4 mm steel pipe. B and C: By compressing the inlet lever, the pressure rises in the container and the perfusate is propelled through the cannula. D: When the clear silicone tubing and cannula are filled with perfusate, the flow is stopped with a clamp and the system is ready for use.
