This protocol creates a PU in the setting of complete SCI. Briefly (as illustrated in Figure 1), all mice with or without complete SCI tolerated the magnets very well, which remained in their original position for the full 12 h (Figures 1c, 1d, 1f, 1h). All the mice developed two circular wounds separated by a bridge of normal tissue (Figure 1e, 1g, 1i). The initial wounding response was similar in mice without SCI (Figure 1e), or with SCI below the SCI site (Figure 1g) or above the SCI site (Figure 1i).
Figure 2 depicts the disappearance of the epidermis by day 3 of post magnet removal, and its reappearance by day 7, albeit with a significantly slower migration in wounds created below the level of the SCI in SCI mice.
The pressure wounds were graded as per previously published criteria12. Figure 3 and Figure 4 depict the healing features in SCI and control non-SCI mice. The SCI group exhibited slower healing, larger scar area, thinner epidermis and dermis, and lower density of proliferating cells (Ki67+ cells), blood vessels (CD31+ cells), and alpha-smooth muscle actin (α-SMA+) in the skin wounds11,12.
When the skin wounds were created above the level of SCI, as shown in Figure 5, no change in healing time, epidermal and dermal thicknesses or scar area was seen when compared to non-SCI controls.
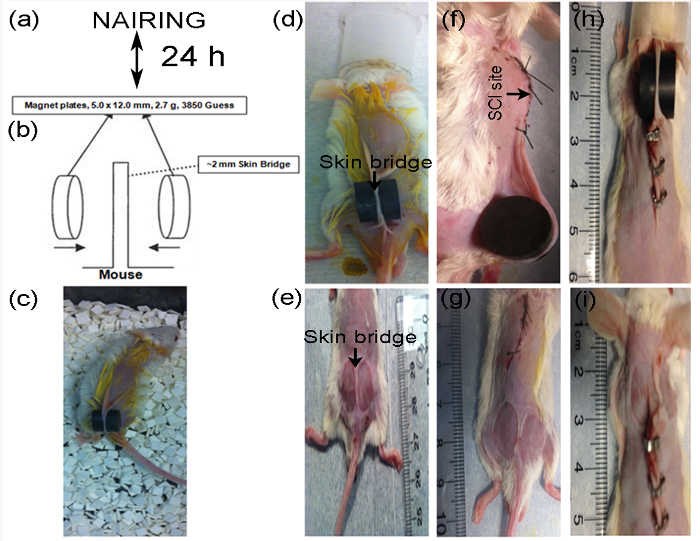
Figure 1: Experimental procedure for creating pressure wounds in non-SCI (n=3) and complete-SCI mice (n = 3). After 1-week habituation in the laboratory, mice were shaved and depilated (a). Schematic of magnetic disc (M) placement (b, modified from Stadler et al.15). Placement of magnetic discs on skin dorsum of a normal mouse and its activity after recovery from anesthesia in the cage (d, c). In SCI mice, discs can be placed below (f) or above (h) the SCI site. The area of magnet-induced skin injury is visible immediately after 12 h of M application, which shows 2 wounds separated by an intact skin bridge in the non-SCI (e) and SCI mice (g, i). Please click here to view a larger version of this figure.
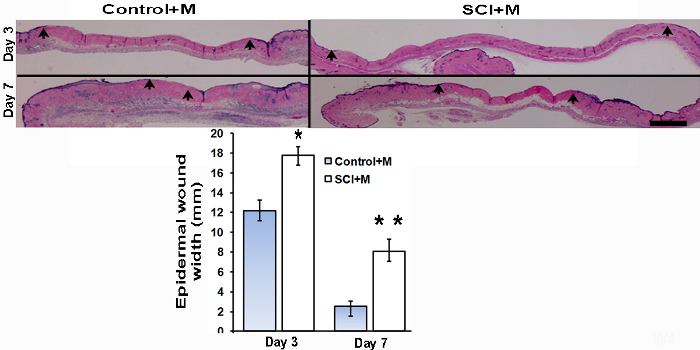
Figure 2: Skin wound histology (H & E stain) and epidermal wound width. On day 3 and day 7 after M application, a set of mice were sacrificed in the non-SCI (Control + M) and complete-SCI (SCI + M) groups to study the early effects M-induced ischemia and then reperfusion. Arrows indicate the epidermal wound edges, located where the epithelial lining thins out and disappears. Scale bar = 1 mm. Epidermal wound width as measured in each group (n = 3 at each time point) is represented in the lower panel bar diagram. Statistical significance determined by Student t-test. *p < 0.05 and **p < 0.01. Data are presented as mean ± SEM (standard error of the mean). This figure has been modified with permission from the Journal of Neurotrauma, 35, 6, 815-824, (2018), published by Mary Ann Liebert, Inc., New Rochelle, NY12. Please click here to view a larger version of this figure.
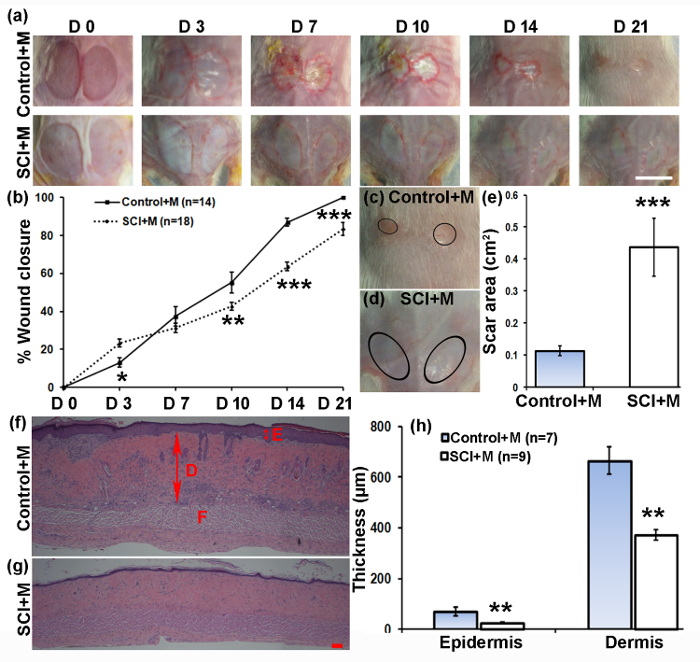
Figure 3: Impact of complete SCI on M-induced PU development and healing. (a) Representative images of skin wounds in non-SCI (Control + M) and complete-SCI (SCI+M) mice after PU induction over the period of 21 days. Scale bar = 1 cm. (b) Quantified wound images showing the fraction of wound closure as a function of time. (c, d) Representative images of healed wounds showing the scar area in non-SCI and SCI mice. (e) Quantified scar area in non-SCI versus SCI mice. (f, g) Representative histology of healed wound skin (H&E staining) showing epidermis (E, double arrows), dermis (D, large double arrows), and fat layer (F). Scale bar = 100 µm. (h) Quantification of epidermal and dermal thicknesses of healed wounds at time of wound closure (21 days for non-SCI, and 35 days for SCI mice). Data are presented as mean±SEM. Statistical significance determined by ANOVA followed by post-hoc Fisher's LSD test and Student's t-test. *p < 0.05, **p < 0.01, and ***p < 0.001. This figure has been reprinted with permission from the Journal of Neurotrauma, 35, 6, 815-824, (2018), published by Mary Ann Liebert, Inc., New Rochelle, NY12. Please click here to view a larger version of this figure.
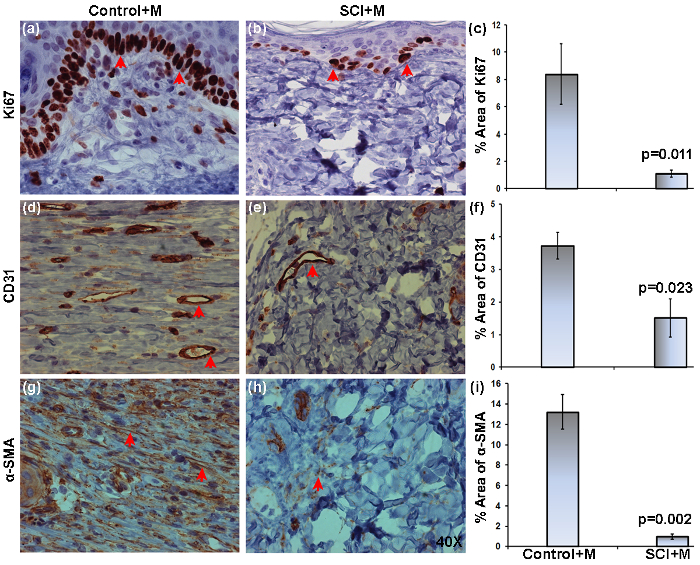
Figure 4: Expression of Ki67, CD31, and a-SMA in skin ulcers of non-SCI and SCI mice. Wound tissues were harvested after wound closure, namely on days 21 (Control+M) and 35 (SCI+M) post-PU induction. Representative images of 5 µm thick sections stained with anti-Ki67, anti-CD31, or anti-α-SMA and visualized with a 40x objective. Representative images of non-SCI (a, d, g) and SCI (b, e, h) mice show the distribution of Ki67+, CD31+, and α-SMA+ (brown stain, red arrows point to some stained areas). The % positive area of expression as obtained by image analysis is compared between the groups (c, f, i). The area was averaged from three 40x fields (two from wound edges and one from wound center) per section (2/mouse, 3 mice in each group). Data are presented as mean ± SEM. Statistical significance was determined by Student's t-test. This figure has been reprinted with permission from the Journal of Neurotrauma, 35, 6, 815-824, (2018), published by Mary Ann Liebert, Inc., New Rochelle, NY12. Please click here to view a larger version of this figure.
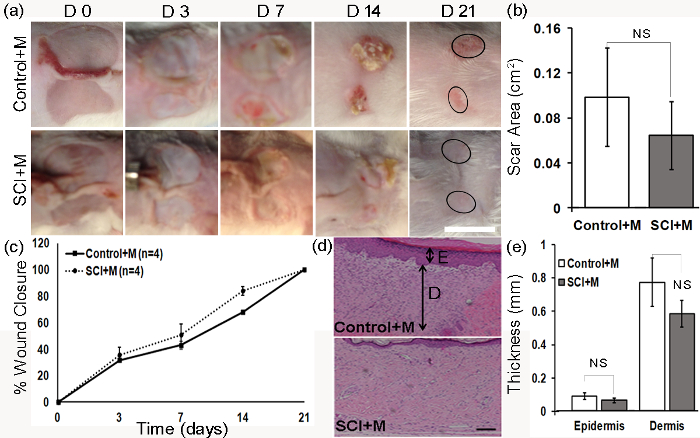
Figure 5: Impact of SCI on development and healing of ulcers above the SCI site. Representative images of ulcers in the non-SCI (Control + M) and SCI (SCI + M) mice over the observation period (a). Scale bar = 1 cm. The scar area on day 21 is represented by circles (a) and values were averaged in non-SCI and SCI mice (b). Quantified wound images showing the fraction of wound closure as a function of time (c). Representative histology of healed skin ulcers showing epidermis (E, small double arrow) and dermis (D, large double arrow). Scale bar = 100 µm (d). Quantification of epidermal and dermal thicknesses of healed skin ulcers at wound closure time (day 21). Data are presented as mean ± SEM. Statistical significance determined by ANOVA followed by posthoc Fisher's LSD test, or Student t-test. NS-statistically non-significant. This figure has been modified and reprinted with permission from the Journal of Neurotrauma, 35, 6, 815-824, (2018), published by Mary Ann Liebert, Inc., New Rochelle, NY12. Please click here to view a larger version of this figure.
Supplementary Figure 1: Motor function in SCI mice was assessed using the BMS score on post-injury day 2 and then weekly. The BMS score at day 2 and week 5 were 0.058 ±0.058 (median 0-no movement, n = 17) and 0.35±0.12 (n = 17, median-0). Data are represented as mean±SEM. This figure has been modified and reprinted with permission from the Journal of Neurotrauma, 35, 6, 815-824, (2018), published by Mary Ann Liebert, Inc., New Rochelle, NY12. Please click here to download this figure.
