RS800CX Technology Set-up
Using the procedure presented here, it is important to highlight that the placement and security of the chest strap is crucial to prevent the strap from falling or moving excessively over the 24 h recording period and consequently, in the collection of an accurate recording. Figure 1 depicts the optimal placement of the heart rate technology, noting that the chest strap and sensor are secure and centered on the youth's sternum (xiphoid process).

Figure 1: Diagram of heart rate technology, depicting optimal placement of chest strap, sensor and watch. Please click here to view a larger version of this figure.
Heart Rate Variability Output Data
Figure 2 depicts the Kubios output of a 24 h heart rate recording for a concussed participant. The image of the raw RR series allows the researcher to visualize change across time, highlighting key time points of increase (e.g., physical activity) or decrease (e.g., resting, sleeping) that are important for the interpretation of data. Time and frequency domain variables represent the overall variability of the physiological signal and the branches of ANS, respectively. Table 1 provides an overview of the units of measurement for time and frequency domain HRV variables and their physiological significance.
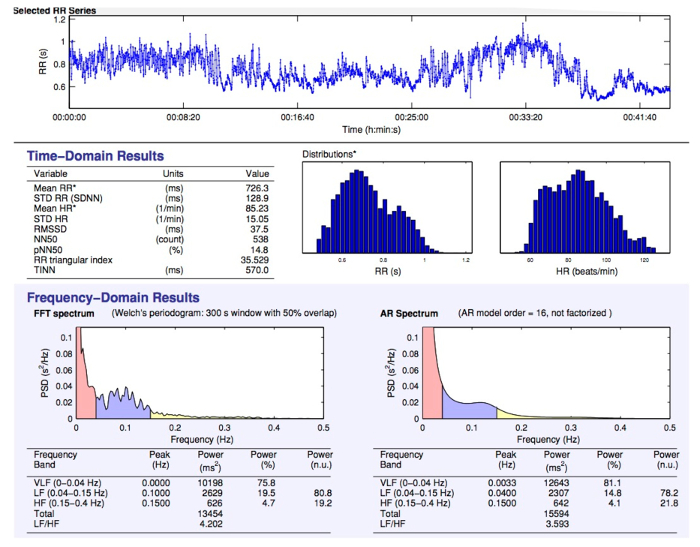
Figure 2: Sample 24 h data output depicting raw RR series, time domain variables and frequency domain variables. Please click here to view a larger version of this figure.
| Variable (units) | Definition | Physiological Significance | |
| Time Domain | |||
| SDNN (ms) | Standard deviation of intervals between heartbeats | Global index of ANS function | |
| RMSSD (ms) | Root mean square of successive differences; calculated through squaring the intervals between heartbeats | Global index of ANS function | |
| pNN50 (%) | Proportion of heartbeat intervals that differ by more than 50 ms | Indicative of parasympathetic activity | |
| NN50 | A count variable; | Indicative of parasympathetic activity | |
| number of pairs of adjacent NN intervals differing by more than 50 ms | |||
| STD HR (s) | Standard deviation of instantaneous heart rate values | Global index of ANS function | |
| Geometric Methods | |||
| RR Triangular Index | Total number of all NN intervals divided by the height of the histogram of all NN intervals | Global index of ANS function | |
| measured on a discrete scale (i.e. the number of all NN intervals divided by the maximum of the density distribution) | |||
| TINN (ms) | Baseline width of the distribution measured as a base of a triangle, approximating the NN interval distribution | Global index of ANS function | |
| Frequency Domain | |||
| HF (ms2) | Power (magnitude) in high frequency range, 0.15-0.4 Hz | Index of parasympathetic activity on heart based on rhythmic respiration cycles | |
| HFnu (%) | HF power in normalized units, as a ratio of the total power; [HF/(HF+LF)] x 100 | Proportion of parasympathetic activity | |
| LF (ms2)* | Power (magnitude) in low frequency range, 0.04-0.15 Hz | Measure of sympathetic and/or parasympathetic activity | |
| LFnu (%)* | LF power in normalized units, as a ratio of the total power; [LF/(HF+LF)] x 100 | Measure of sympathetic and/or parasympathetic activity | |
| LF/HF (ms2)* | Ratio of low frequency power to high frequency power | Measure of sympathetic and/or parasympathetic activity | |
| Total power (ms2) | Variance of all RR intervals | Overall magnitude of variability within ANS; ability of ANS system to be flexible and adaptable | |
Table 1: Description of time domain and frequency domain HRV variables.
NOTE: "*" denotes cautionary interpretation of LF-related variables, as the clinical usefulness and validity of this measure is controversial. It has been postulated that LF is not representative of sympathetic autonomic modulation27, in addition to having a poor relationship to sympathetic nerve activation28. Thus, it is challenging to decipher the physiological basis of this measure.
Visualizing Subjective and Objective Findings
Given the novelty in 24 h recording methodology, visualization of findings across the recovery trajectory is key to interpretation of findings with respect to mapping "clinical recovery" with potential "physiological recovery". It is important to note that consistency is maintained regarding the investigator that interprets visual trends in order to ensure reliability. In this particular protocol, the primary author, well versed in neurophysiology, interpreted all aggregate trends. The interpretation of these trends was then reviewed within an interdisciplinary context of experts in pediatric concussion, theoretical physiology and exercise physiology. Thus, a well-informed approach to visualizations is key to making preliminary inferences regarding the recovery trajectory. Figure 3 depicts the relationship between pNN50 and PCSI total score across days post-injury, stratified by sex. Within a longitudinal research setting, collecting repeated measures data could provide rich HRV data. Figure 3 is an example of the recovery trajectory when comparing youth males to youth females. Here, the recovery trajectory appears to be similar within both males (A) and females (B), whereby an initial decrease is found until day 30, followed by increases until day 75/90 for males and females respectively, and then followed by a plateau.
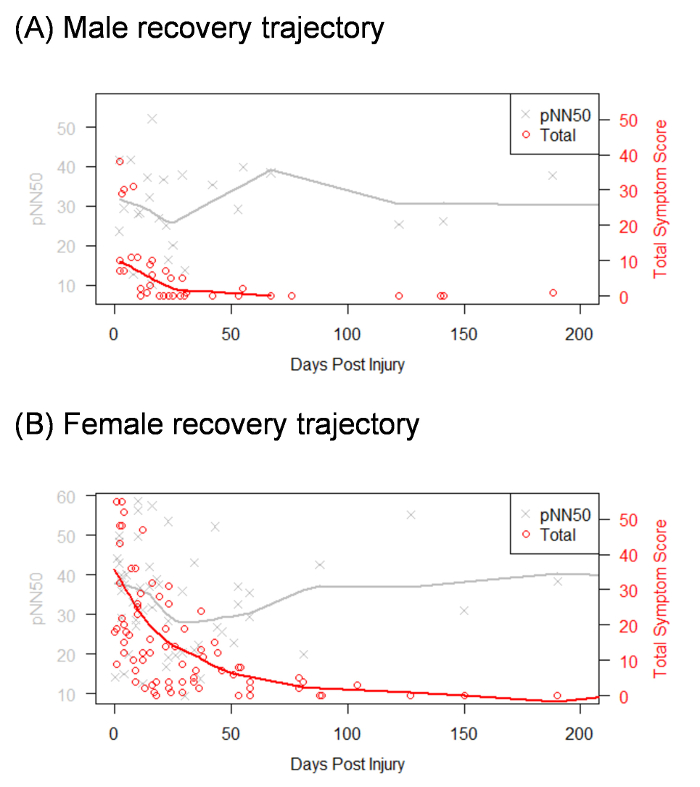
Figure 3: Visualization of recovery trajectory across days post injury, stratified by sex. Please note that "Total" in the legend box reflects the total PCSI score. Please click here to view a larger version of this figure.
