All animal experiments were performed according to the National Institutes of Health guidelines, with the authorization number: AL/60/67/02/13.
1. Recipient Preparation
- Chemically induce diabetes in recipient rats.
- Inject 75 mg/kg of streptozotocin (STZ, in sterile 0.1 M citrate buffer, pH 4) intraperitoneally to rats10.
NOTE: For the transplantation studies, 6 week-old Lewis strain rats, weighing 150-190 g were used. - Check the diabetes status by daily blood glucose measurements during the first four days. Inject long-acting insulin 6 U/day subcutaneously when rats exhibit glycemia over 2 g/L to prevent diabetes complications and weight loss, until insulin pellet implantation.
- Include rats in the cohort when two measures of tail vein blood glucose are >4-5 g/L for 2 consecutive days, and C-peptide level is <200 pM. Measure glycemia using a glucometer and C-peptidemia by an enzyme-linked immunosorbent assay (ELISA).
- Implant insulin pellets under the skin (see 1.2).
NOTE: Chronic insulin therapy allows better glycemia regulation and avoids diabetic complications (which exacerbate oxidative stress at the transplantation site)11. Furthermore, the therapy conserves the diabetic state along with a normal growth curve (without usual weight loss observed in a diabetic animal). This can result in a bigger omental fat pad, which is ideal for carrying out transplantation.
- Inject 75 mg/kg of streptozotocin (STZ, in sterile 0.1 M citrate buffer, pH 4) intraperitoneally to rats10.
- Implantation of insulin pellets
- Anesthetize the rat using gas anesthesia (3% isoflurane in 500 mL/min O2) and place the rat in the prone position.
- Verify anesthesia status by checking the absence of reflex (paw pinching). Clean the neck using povidone iodine, and shave the area using a razor blade. Apply povidone iodine again and let it stand for 3 min.
- Place 1.5 insulin pellets (3 Units (U)/200 g rat) in a 1:5 diluted povidone iodine solution to sterilize the pellets. Pierce the neck skin using a 16 G trocar and insert the pellet using the furnished guide and stylet. Retrieve the guide and stylet and stitch a single point. Use povidone iodine to clean the stitch.
NOTE: No post-surgical pain management was necessary as the intervention was comparable to a single subcutaneous (SC) injection. - Let the rat recover from anesthesia and ensure that rats have access to food to avoid hypoglycemia.
- Measure the efficiency of pellet by measuring glycaemia decrease after implantation.
- Check the pellet efficiency by monitoring glycemia level every week for 1 month.
- Include rats in the cohort when a measure of tail vein blood C peptide level is maintained under 200 pM 1 month after insulin pellet implantation.
NOTE: Checking C-peptide levels is mandatory to evaluate animals at baseline before transplantation and to confirm their diabetic state. Low C-peptide regeneration always occurs during follow-up. The lowest C-peptidemia is indicative of the lowest regeneration.
2. hOMING: Intra-omental Matrix Islet Filling
- Islet-matrix mixture preparation.
- Prepare the viscous islet carrier in a laminar flow hood. Dissolve alginate powder in sterile PBS at a concentration of 1.5%. Sterilize the preparation by passage through a 0.22 µm filter. Prepare 400 µL per recipient.
NOTE: Any kind of hydrogel with a viscosity suitable for injection through a 21 G needle can be used. - Isolate islet from healthy Lewis rats (200-250 g) as previously described12.
- Count islet number in islet equivalents (IEQ) (one IEQ is considered equivalent to a pancreatic islet with a diameter of 150 µm)13.
- In a laminar flow hood, prepare aliquots of 7660-islet equivalent (IEQ) in a 1.5 mL tube.
- Wash islets aliquots with 500 µL of CMRL (Connaught Medical Research Laboratories) medium free of fetal bovine serum.
- Pellet islets by centrifugation (2 min at 500 x g and 4 °C). Discard the supernatant.
- Add 150 µL of alginate hydrogel carrier over the islets, mix carefully by pipetting up and down and place the mix on ice.
- Prepare an atraumatic 21 G needle and a 1 mL syringe without dead volume by loading 150 µL of empty alginate into the syringe.
- Fill the syringe with the mixture of islets and alginate (150 µL, total volume 300 µL). Keep the syringe on ice.
- Prepare the viscous islet carrier in a laminar flow hood. Dissolve alginate powder in sterile PBS at a concentration of 1.5%. Sterilize the preparation by passage through a 0.22 µm filter. Prepare 400 µL per recipient.
- Surgical procedure
- Sterilize surgical instruments using cold sterilization (2% Steranios for 20 min).
- Anesthetize the rat using isoflurane anesthesia and place the rat in the prone position.
- Shave the neck area using a razor blade and sterilize the area with povidone iodine. Let the iodine stand for 3 min.
- Make an incision using a scalpel and remove the 1.5 insulin pellets using forceps. Close the skin using one or two single stitch points. Do not remove the rat from anesthesia.
NOTE: After 1 month, the pellet can be friable as some fibrotic tissue can wrap as pellets; use scissors to properly dissect it. - Place the rat in the supine position. Shave and sterilize (with povidone iodine) the peritoneal area. Let the iodine stand for 3 min.
- Create a 1.5 cm laparotomy just under the sternum using a scalpel. Place wet-sterile gauze around the incised area.
- Identify the omentum that is the fat pad localized next to stomach. Use forceps to carefully catch the omentum, pull it gently out of the peritoneal cavity, and spread it on the gauze.
NOTE: The omental tissue extends from the spleen to the duodenum and attaches at its mid-point to the stomach. The normal omentum of diabetic rats receiving insulin therapy is approximately 2 cm² when spread on the gauze. - Hydrate the omental tissue well using 2 mL of pre-warmed 37 °C sterile saline. Use small curved forceps to manipulate the tissue and penetrate the omental edge with the needle between the omental layers. Insert the needle entirely.
- Start the injection of the islet preparation slowly and carefully move the needle backward to inject the islets in several places (as lines). Prior to withdrawing the needle, ensure that the hydrogel has stopped exiting the needle to avoid the loss of the dispersed islets.
- Repeat this manipulation as needed to inject the entire contents of the syringe using different entry points to distribute the islets throughout the omental tissue.
NOTE: In rats, four to five injections are generally needed. - Check that islets are not clustered in the syringe at the end of the injections.
NOTE: If some islets are still visible, it is possible to withdraw the needle from the syringe, fill the syringe directly with 100 µL of empty hydrogel, and reconnect the needle. A second round of injection can be done to flush out the remaining islets. - Use sterile saline again to hydrate the omental tissue and the wall of the laparotomy. Use forceps to carefully replace omentum in the abdominal cavity.
- Inject 2 mL of pre-warmed sterile saline into the abdominal cavity to rehydrate the rat.
- Close the muscle wall using a continuous thread suture. Then stitch the cutaneous layer with single stitch point (point-by-point).
- Inject meloxicam (1.5 mg/kg) subcutaneously as an analgesic for 5 days once a day.
- Place the rat in a cage on a heating pad until recovery from anesthesia. Repeat the procedure for all the recipient rats.
- Measure the blood glucose after transplantation every day. If glycemia is >2 g/L, inject 6 U of long-acting insulin subcutaneously once a day.
- Assess graft function by glycemia and c-peptidemia monitoring over 1 or 2 months.
NOTE: In cases of successful transplantation, glycemia should stabilize within 2-5 days after transplantation, and rats can be taken off insulin.
3. Omental Graft Explantation
NOTE: This procedure will permit the confirmation of good graft function. After retrieval of a functional graft, rats should return to a diabetic state. This step is performed after 1 or 2 months of metabolic follow-up.
- Anesthetize the rat with gas anesthesia and place it in the supine position.
- Shave the peritoneal area and sterilize it using povidone iodine for 3 min.
- Create a 1.5 cm laparotomy just under sternum using a scalpel. Place wet-sterile gauze all around the incised area.
- Identify the omentum, which is next to the stomach. Use forceps to carefully spread it on the gauze.
- Use scissors to excise the omentum. Start from the part that adheres onto the pancreas tail (next to the spleen). If bleeding occurs, use dry sterile gauze to stop it.
- Continue excision along the part attached to the stomach and retrieve the omentum.
NOTE: At this location, gastroepiploic arteries (Figure 1) can cause a large amount of bleeding if they are accidentally cut. Artery incisions are inevitable to retrieve the graft, but bleeding can be managed using forceps and gauze. If an accidental cut happens, compress firmly with dry gauze and maintain the compression for at least 1 min. The bleeding should stop. If not, use clips or use an electric bistoury to cauterize the vessels.
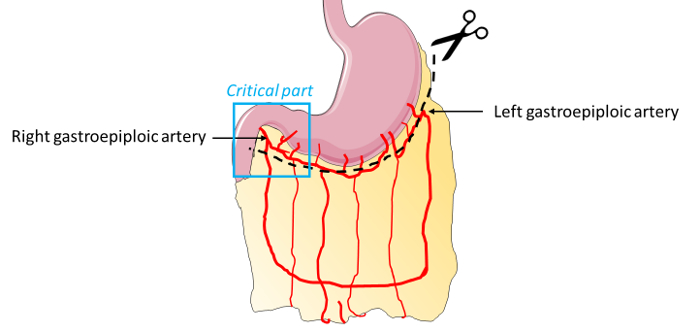
Figure 1: Omental artery distribution. For omentum graft explantation, the critical area composed of gastroepiploic arteries is represented in blue. During resection of this part of the omental tissue, attention must be to be paid to the right gastroepiploic artery section. Compression, ligature, or cauterization can be used to limit bleeding. Please click here to view a larger version of this figure.
- Check if any bleeding persists. If not, inject 2 mL of pre-warmed saline, close the rat, and process as previously described.
Explanted animals return to a diabetic state. Insulin injection (6 U/SC/day) is then mandatory to assure well-being of animals. - Euthanize the rat 10 to 12 days after explantation using an overdose of pentobarbital (182.2 mg/kg).
4. Histological Analysis: Hematoxylin and Eosin Staining
- Fix the retrieved omenta using 4% paraformaldehyde (PFA) and embed in paraffin.
- Cut sections 4 µm in thickness and apply hematoxylin and eosin stain for morphological evaluation of the transplant.
5. Statistical Analysis
- Determine statistical significance using statistical analysis software and repeated measures analysis of variance (ANOVA) with Tukey’s honest significance difference test as a post hoc test. Represent p values as: *p < 0.05; ** p < 0.01; *** p < 0.001.
The hOMING method permits the avoidance of intravascular implantation and the confinement of islets in an organ. A maximum time of 8-10 min is required for the entire islet implantation procedure, including anesthesia, which a timeline comparable to classical liver transplantation.
To study the way islets are distributed inside the omental tissue, dextran beads were transplanted using the hOMING method (Figure 2). One day after implantation, rats were sacrificed, and omental tissues were retrieved for histological analysis. Hematoxylin and eosin staining revealed a uniform distribution of the beads throughout the tissue (Figure 2, bottom right). Very often, beads were close to blood vessels and were well-implanted in the fat tissue. Immediately after implantation, an inflammatory reaction occurs around the beads, resulting in tissue rearrangement to nest the islets in the tissue.
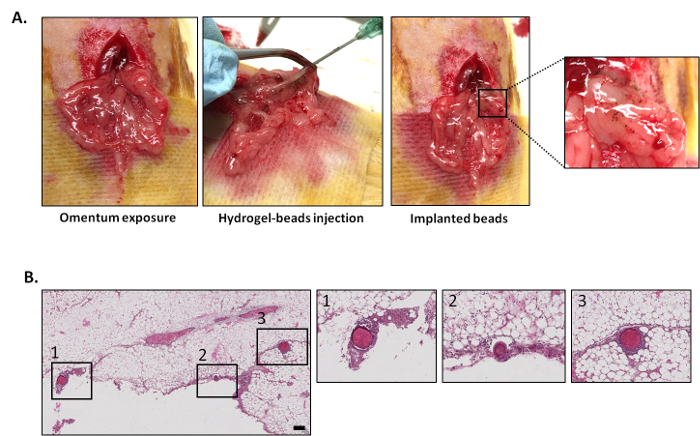
Figure 2: Description of hOMING technique and bead distribution through the omental tissue one day after implantation. (A) Illustration of the hOMING technique. After organ exposure (A, left), the islet-hydrogel mix (replaced here by blue-colored dextran beads for better visualization) was carefully injected in the tissue using an atraumatic needle (A, middle). Beads implanted in the tissue are visible (A, right). (B) Hematoxylin and eosin staining of omentum explanted 1 day after bead injection. Beads are found in the tissue with a uniform distribution. Scale bar = 100 mm. Please click here to view a larger version of this figure.
To validate this technique, we performed isogenic studies using Lewis rats (n=8). Diabetic rats receiving islet transplants (7660 islet equivalent, IEQ) per kg rat body weight using hOMING were monitored for glycemia and C-peptidemia for two months. Glycemia was controlled by implantation of insulin pellet (as attesting to the first drop in glycemia observed in the Figure 3A). Graft function was reflected by glycemia of approximately 2 g/L and C-peptidemia >500 pM. Before transplantation, rats were diabetic (glycaemia >5 g/L and C-peptidemia <200 pM). After transplantation and insulin pellet retrieval, glycemia maintenance and normalization was observed just 3 days post-hOMING transplantation and was maintained until graft retrieval (p < 0.05 compared to pre-transplant levels). After omental explantation, glycemia rose again to the pre-transplant level, attesting to the functionality of islets that were transplanted by hOMING (Figure 3A). The C-peptidemia pattern was exactly the opposite, with low to undetectable levels before the graft, followed by an increase and maintenance at this increased level throughout the course of the study (p <0.05), and, after omental explantation, a decrease to pre-transplant levels (Figure 3B). Analysis of the explanted omentum by histology revealed highly re-vascularized islets, most likely as a result of their proximity to blood vessels (Figure 3C).
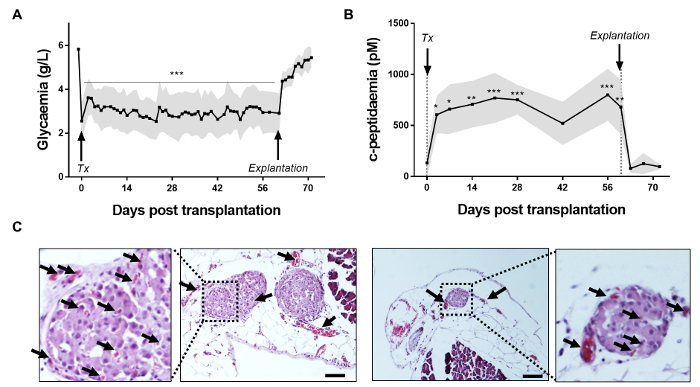
Figure 3: Two-month metabolic follow-up of rats receiving hOMING and graft assessment. (A) Glycemia measurement and (B) C-peptide assessment after hOMING using alginate as an islet carrier (Tx: Transplantation and insulin pellet retrieval; Explantation: Explantation of the omentum). Grafts are functional, as is shown by the maintenance of normoglycemia after insulin pellet retrieval and increase in C-peptidemia after islet implantation. Gray shaded areas represent the minimal and maximal recorded values at each time point. (C) Hematoxylin and eosin staining of an omental section after islet transplantation using the hOMING method. Islets are well-integrated into the tissue two months after implantation without any surrounding fibrotic tissue. Vessels have grown around and inside islets, as shown by the arrows, and thus completely restore islet function. Morphology of the islets also seems well-preserved. Scale bars = 50 µm. (n = 8) (*p < 0.05; ** p < 0.01; *** p < 0.001 determined using repeated measures analysis of variance (ANOVA) with Tukey's honest significance difference test as a post hoc test). Please click here to view a larger version of this figure.
