At present, 20 participants have been recruited to the study. For the participants in the study group, the smart digital garment and wristband are used as monitored tracking devices for most of the variables measured. Some variables, such as food intake, sugar levels, and weight, are entered manually by the patient. The patients in the study group have to wear the wristband most of the day and the smart digital garment twice a week for 30 min for 6 weeks while they are in the CR facility and 6 more weeks at home.
To perform the study, the wristband is used to measure all the physiological variables needed, and the smart digital garment is used for performing ECG. Both devices transmit the measured data to a smartphone that operates an application designed to collect data and transmit it directly to the system. The system is programmed to analyze and then execute the material analyzed (Figure 1). A dashboard facilitates the collection and visualization of the raw and analyzed data (Figure 2).
A combination of commercially available wearable tools is used with a system capable of evaluating and quantifying the various variables designed especially for the assessment of heart patients who use these devices. To this end, changes in physiological signals such as heart rate, sugar, and sleep, as well as nutrition data and more, are measured. In the course of the various activities, it is possible to assess the activity or inactivity of the patient on a daily basis, to know the patient's condition in real-time. After analyzing the data by the system, an immediate evaluation can be done by the medical team at the center who observes the results that appear on the dashboard (Figure 2 and Figure 3). The team has the ability to react immediately to any deviation from normal. The patient is under observation all day, and the coordinator is in contact with the patient to encourage them to continue keeping up their activity levels or to check why there is no activity by sending the patient daily to monthly graphic reports, and this is done throughout the 3 months' program (Figure 5 and Figure 6).
At this stage, initial observations, comments, and responses from participants show a clear preference for home digital telemedicine. Everyday contact via chat and the ability to practice throughout the day rather than being on a rigid schedule gives them an incentive to practice and be rehabilitated. Patients report a decrease in anxiety, and they are more confident and relaxed and sleep better at night for more time. The various indices measured also indicate an improvement; a decrease in general and abdominal fat levels and increased muscle mass was also observed, but this cannot yet be assessed statistically.
The results obtained from this study should support an alternative, home-based approach to enhance the long-term therapeutic efficacy of cardiac rehabilitation, especially for those patients who are unwilling or unable to participate in traditional rehabilitation programs.
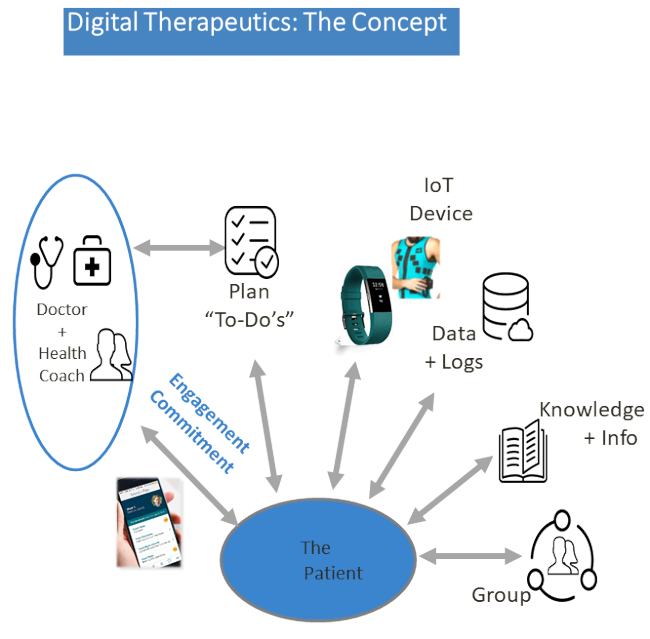
Figure 1: The digital program concept. The program registers the clinicians, as well as coaches and onboard patients, immediately. It is tailored to address the range of the medical team's needs concerning physical activity, behavioral health, medication, and nutrition via the application video and audio communication channels between patients and coaches.

Figure 2: The platform dashboard. Patients, wearing a special wristband and garment, will have reciprocal multichannel access to their coach via their mobile phone for a personal plan and video and audio guidance. The coach is able to track the patient's activity at all times, leading to more precisely followed care plans and healthier decisions. Please click here to view a larger version of this figure.
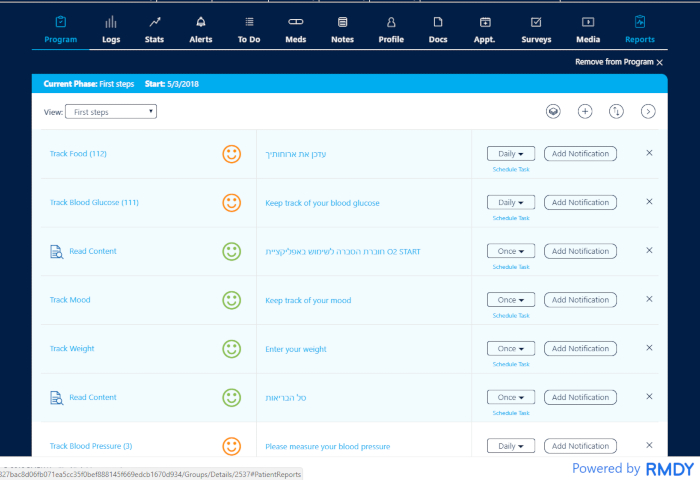
Figure 3: One patient's program. The patient is in observation all day long. The coordinator/coach is able to track the patient's activity at all times and is in contact with the patient to encourage them to continue their activity or to check why there is no activity. The multidisciplinary team has the ability to react immediately to any deviation from normality. Please click here to view a larger version of this figure.
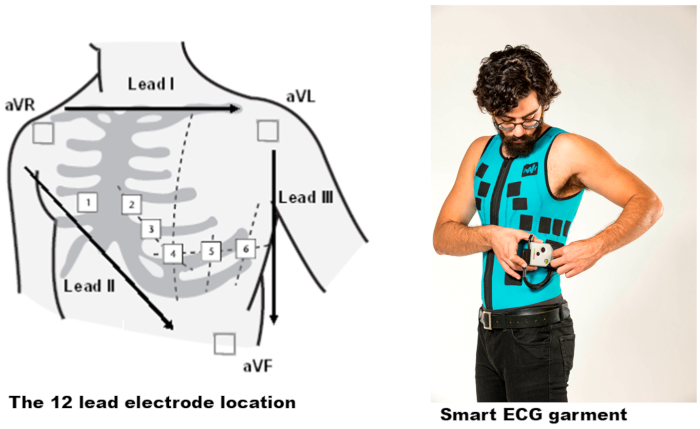
Figure 4: The Master Caution garment and the electrodes' locations. The standard limb leads I, II, and III each record the differences in electrical potential between two limbs. An additional six unipolar leads record the electrical potential difference between an exploring electrode and an indifferent electrode located centrally in the chest and computed from the average of the limb recordings. Please click here to view a larger version of this figure.
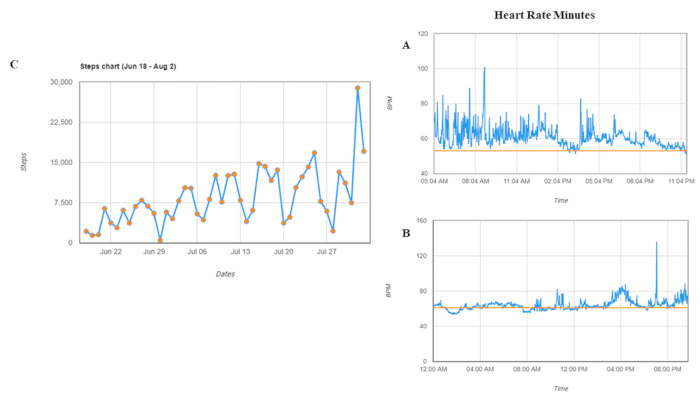
Figure 5: Graph reports for one patient. (A) A day of an active person. (B) A day of a sedentary person. (C) Average resting heart rate. Patients can be followed per day and per month. Heart rate = heart rate per minute. Please click here to view a larger version of this figure.
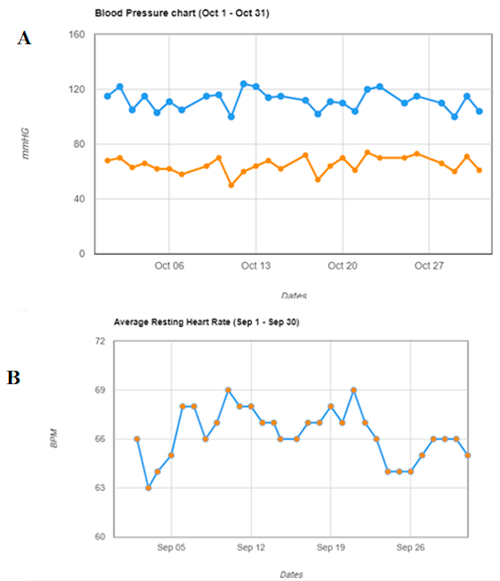
Figure 6: Graph reports for one patient. (A) Blood pressure. (B) Steps chart. Patients can be followed per day and per month.
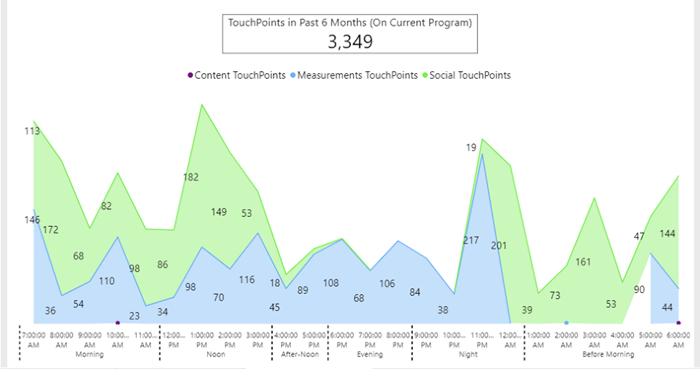
Figure 7: Daily behavior of one patient as aggregate activity during 6 months. Patient's engagement and frequency points of contact, through the app, between him and his coordinator. The green color shows the extent and time of communication between the coordinator and the patient displayed as touchpoints. The blue color indicates the number of measurements of the various indices as sent by the patient throughout one day, displayed as touchpoints.
