Head position during IN administration is a major influence on the efficiency of drug delivery to the brain. Here we described the head down-and-forward position using a mouse positioning device for the IN administration of a brain-targeting peptide-siRNA formulation for the delivery of the mixture to the mouse's CNS. To verify delivery through the IN route, we used the RVG9R peptide, previously shown to efficiently bind to neuronal cells both in vitro and in vivo14,16.
We first tested nose-to-brain delivery of the RVG9R peptide labeled with Alexa Fluor 488 (RVG9R-A488) by using the mouse positioning device described here. At 48 h postinoculation, various organs, including the brain, the sinus, lungs, the liver, the spleen, and kidneys were excised to measure tissue-associated A488 fluorescence. A488 alone, or a control peptide (RVM9R-A488)14 that does not bind nAchR, were used as negative controls. As expected, neither A488 nor RVM9R-A488 were detected in any of the organs at 48 h postinoculation (Figure 3A, left). On the other hand, a strong fluorescent A488 signal was detected exclusively in the brains of the RVG9R-inoculated group. In addition, we compared this mouse placement position to the supine position method that has been used previously17, as well as to the awake method, for efficacy. We inoculated a fixed amount of RVG9R-A488 (100 µg) and assayed biodistribution at 48 h postinoculation. The results indicated that positioning the mice head down-and-forward improved the penetrance and deposition of RVG9R-A488 throughout the brain tissue (Figure 3A, right). In contrast, the animals inoculated in a supine position resulted in the delivery of RVG9R-A488 to the brain but not as strong as seen with the positioning device method. To further confirm siRNA delivery to the brain, we performed full-brain scanning after a single IN administration of RVG9R complexed to 400 pmol (5.2 µg) of Cy5-labeled siRNA. In contrast to PBS or RVM9R, complexing with RVG9R resulted in a strong accumulation of siRNA in major brain regions, including the olfactory bulb, the cortex, the hippocampus, the thalamus, the hypothalamus, the midbrain, and the cerebellum (Figure 3B).
Finally, we employed RT-qPCR analysis to verify the intracellular delivery of functional siRNA targeting the superoxide dismutase-1 (SOD1) gene. Mice were inoculated intranasally for 3 times on consecutive days with RVG9R:siSOD1 (13.2 µg of siRNA), and the SOD1 mRNA expression was analyzed 24 h after the last inoculation. RVG9R:siSOD1 administration resulted in a substantial reduction of the SOD1 expression in the olfactory bulb (63%), the cortex (47%), the hippocampus (61%), the thalamus (53%), the hypothalamus (55%), the midbrain (39%), and the cerebellum (30%) (Figure 4). In conclusion, the use of a positioning device enables an easy IN inoculation of RVG9R-complexed siRNA in mice, resulting in brain-specific siRNA delivery inducing functional silencing of the target gene.
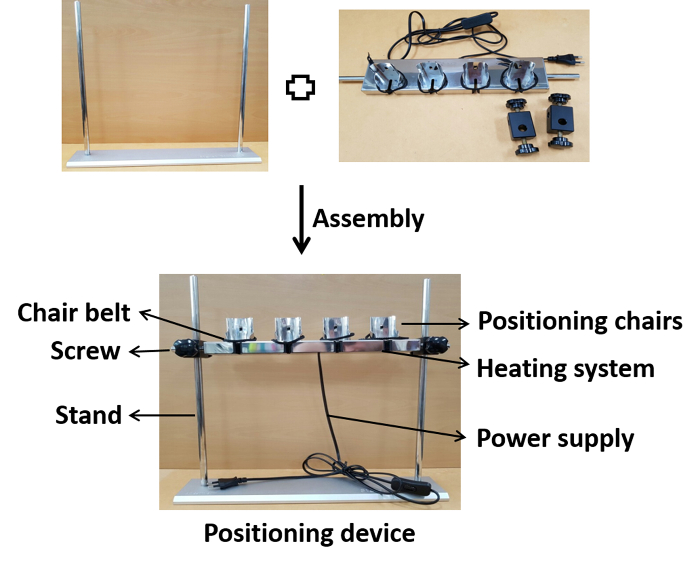
Figure 1: Photographic presentation of the device assembly. The positioning chairs are assembled on the stand at the appropriate height with screws. After the assembly, the device is connected to a power supply for heating to the physiological temperature during inoculation. Please click here to view a larger version of this figure.
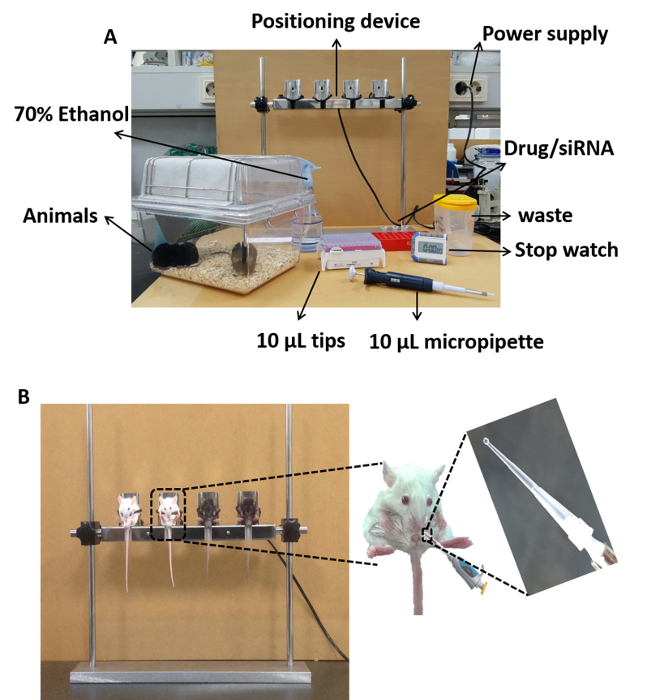
Figure 2: Photographic presentation of the IN inoculation procedure using the positioning device. (A) Experimental equipment required for the IN inoculation. (B) Animals in the head down-and-forward position seated on the device (left) and the deposition of a 2 µL droplet for IN inoculation (right). Please click here to view a larger version of this figure.
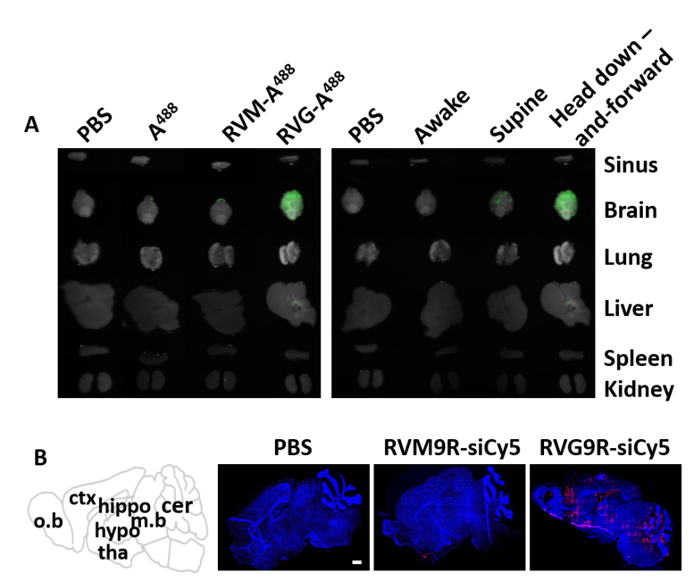
Figure 3: Distribution of fluorescently labeled peptide and siRNA after IN administration. (A) Biodistribution of intranasally inoculated RVG9R peptide at 48 h after a single IN inoculation. The brain and other peripheral organs were evaluated for the presence of fluorescence in mice inoculated with saline (PBS), A488, RVM-A488, and RVG-A488 (left). Imaging of the mice treated as mentioned above while they are awake, in the supine position, and in the mouse positioning devise in the head down-and-forward position (right). (B) Biodistribution of the RVG9R:siRNA complex in the brain (n = 3 per group). The distribution of Cy5-labeled siRNA was visualized in full brain cryosections with a confocal laser microscope in animals inoculated with saline (PBS), siRNA complexed with control peptide (RVM9R-siCy5), or the brain-targeting peptide RVG9R (RVG9R-siCy5). The scale bar represents 1 mm. Abbreviations: o.b = olfactory bulb; ctx = cortex; hippo = hippocampus; hypo = hypothalamus; tha = thalamus; m.b = midbrain; cer = cerebellum. Please click here to view a larger version of this figure.
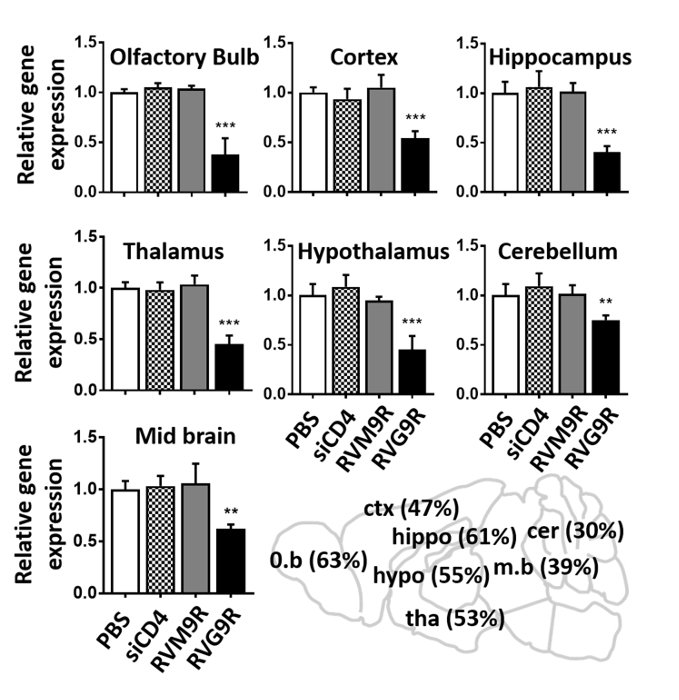
Figure 4: IN application of RVG9R:siSOD1 induces target gene silencing in multiple regions of the brain. qPCR analysis for murine SOD1 mRNA in indicated brain regions 24 h after the last IN inoculation of saline (PBS), RVG9R:siCD4 (siCD4), RVM9R:siSOD1 (RVM9R), and RVG9R:siSOD1 (RVG9R). The relative SOD1 silencing in the olfactory bulb, the cortex, the hippocampus (upper), the thalamus, the hypothalamus, the cerebellum (middle), and the midbrain (lower) is shown. Data represent the mean ± SD relative to GAPDH after normalizing with the corresponding data of saline-treated mice (n = 3 per group). The cartoon depicting the percentage of SOD1 mRNA in the indicated brain region after the IN inoculation is shown (lower right). **P < 0.01, ***P < 0.001. Abbreviations: o.b = olfactory bulb; ctx = cortex; hippo = hippocampus; hypo = hippocampus; tha = thalamus; m.b = midbrain; cer = cerebellum. Please click here to view a larger version of this figure.
