Acquisition of thermographic images and macroscopic assessment to determine whether BST exhibits laterality may be performed within 2 min in most patients. Most acute WS patients exhibit laterality of BST at multiple locations. Some patients exhibit laterality of BST throughout the body (Figure 2A), whereas some exhibit laterality only in a few locations (Figure 2B). The warmer side, as determined by BST, is ipsilateral to the location of WS (Figure 2D,E). Importantly, however, a WS patient with a very small infarction may not exhibit laterality of BST (Figure 2C,F). When a patient does not exhibit a central nervous disorder (e.g., auditory vertigo), laterality of BST is typically not observed (Figure 1). However, when a patient exhibits vascular stenosis, BST may be lower in the extremities with vascular stenosis than in extremities on the contralateral side. Laterality of BST is observed in only one limb in nearly all patients with vascular stenosis. However, patients may exhibit vascular stenosis in both the upper and lower limbs (Figure 3).
The precise degree of BST can be analyzed with dedicated software (Figure 4). This analysis may be required when the laterality of BST is not apparent macroscopically, especially on the face and trunk, because lateral differences in the faces and trunks of WS patients tend to be smaller than those of the extremities in such patients7.
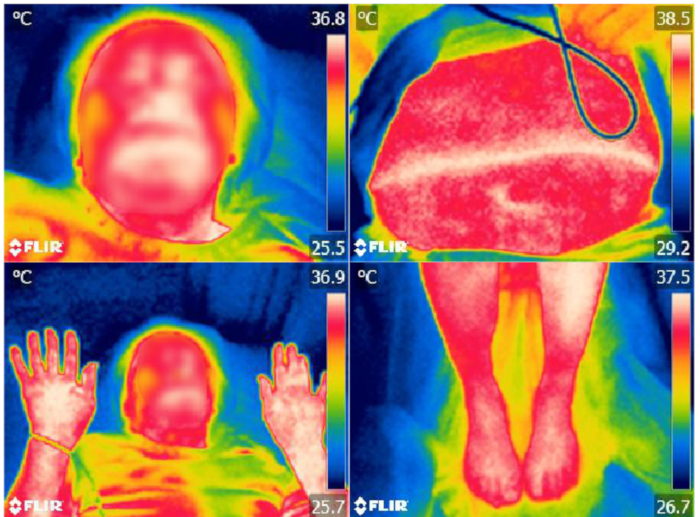
Figure 1: Thermographic images of the face, bilateral palm, abdomen, and bilateral foot of a patient with auditory vertigo. Laterality of BST is not detected. The patient's face is blurred to protect privacy. Please click here to view a larger version of this figure.
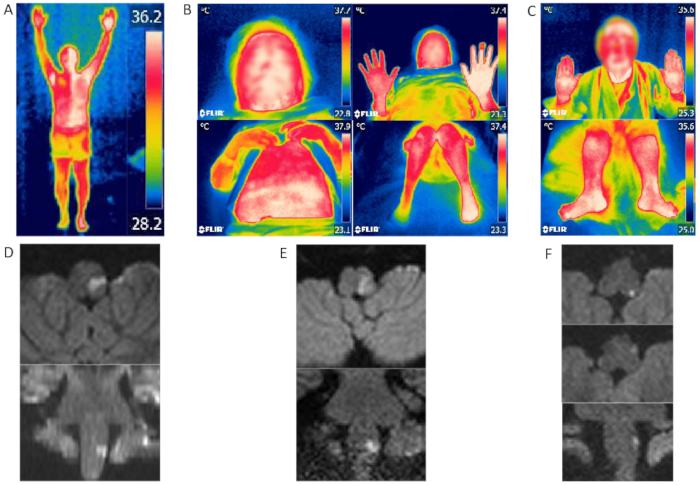
Figure 2: Thermographic images and MRI findings of WS patients. (A, D) WS patient with laterality of BST throughout the body. The warmer side of the patient's body is ipsilateral to the infarction. (B, E) WS patient with laterality of BST of the upper and lower limbs. The warmer side is also ipsilateral to the infarction. (C, F) Brain MRI/diffusion-weighted imaging of this patient revealed a very small high-intensity lesion at the edge of the lateral medulla, but no lateral difference in BST. Patients' faces are blurred to protect privacy. Figure 2B-F were modified from Takahashi et al.7. Please click here to view a larger version of this figure.
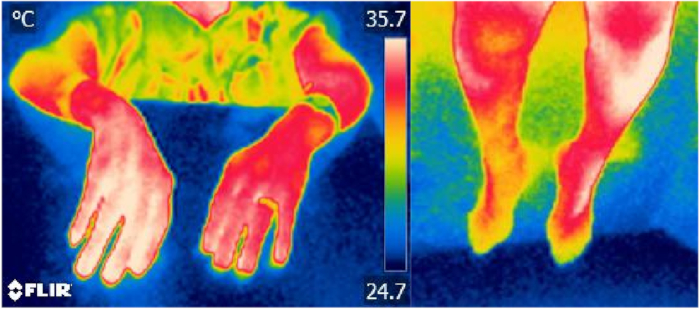
Figure 3: Left upper and right lower extremities of a patient with arterial sclerosis and vascular stenosis. Arterial sclerosis and vascular sclerosis diagnoses were based on ankle-brachial index; thermography reveals higher BST on the contralateral side. Please click here to view a larger version of this figure.
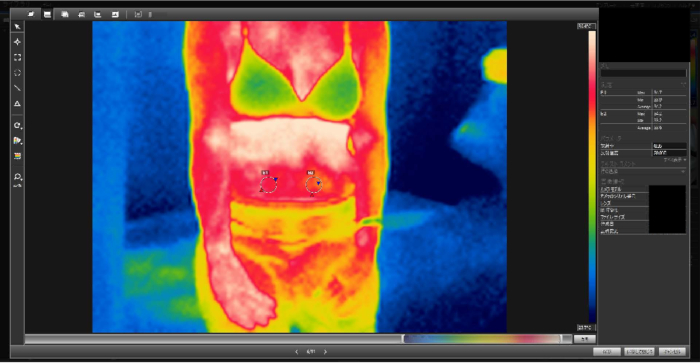
Figure 4: Laterality of BST in the abdomen of a WS patient. Results were equivocal macroscopically, but analysis by ellipse measurement in the analysis software showed a 0.6 °C discrepancy in the average BST between the right and left sides of the abdomen. Please click here to view a larger version of this figure.
