The H2052/484 orthotopic model
Orthotopic MPM models by intra-thoracic injection of cultured cancer cells, especially H2052/484 cells are relatively easy to setup. The different steps described above only require modest cell culture knowledge and the surgery steps are accessible to moderately trained animal experimenters. Nude mice and cells should be manipulated under sterile conditions to maximize the outcome of the implantations. By carefully following this protocol, which involves short anesthesia and minimal surgery, we encountered only 1 death among 266 mice injected with different MPM cell lines. No pneumothorax or intra-pulmonary implantations of tumor cells were observed among these 266 mice carefully injected as described. Specifically, the orthotopic tumor development rate of the H2052/484 cell line is high since 93.8% of injected mice developed tumors (n = 118). H2052/484 tumors can be detected by PET/CT imaging from 14 days after injection and the median duration of the experiment according to our endpoint criteria was 31 days in a representative experiment21. As we described in this other study21, the tumors were localized in the thoracic cavity, freely distributed or attached on the lungs, the thoracic muscles, the aortic arch or the inferior vena cava. Metastases were not found.
MPM monitoring by [18F]FDG-PET/CT imaging
Orthotopic MPM were monitored weekly by combined PET/CT imaging with the widely used radiotracer [18F]FDG that accumulates in highly metabolic tumors. Longitudinal anatomical CT scans allowed visualizing the impact of MPM development on the morphology of lungs. Automatic segmentation of highly contrasted lungs on CT scans is simple due to their low density as compared to surrounding tissues. 3D renderings give an overview of the localization of tumors and longitudinal volumes of lungs can be extracted (Figure 2A). Lung volumes measurements by CT decreased significantly over time after MPM injection of mice with intrapleural (ipl) H2052/484 tumors (Figure 2B). Indeed, MPM tumors grow inside the pleural cavity and create pressures on the lungs, reducing their volumes. Correlation analyses demonstrated that lung volumes were inversely correlated to the time of monitoring with a coefficient of determination R2 of 0.8 (Figure 2C). Altogether, these data show the reliability of CT scan to monitor the development of this MPM model.
Combined with CT, a [18F]FDG-PET scan provides additional and valuable information on the metabolic status of MPM tumors. While sometimes it can be complicated to interpret CT and PET scans images by themselves, especially at early time points, a combination of both modalities gives further robustness to diagnosis. Indeed, representative longitudinal [18F]FDG-PET/CT monitoring performed between 10 days and 44 days of a mouse with ipl H2052/484 tumors shows that tumors begin to be distinguishable 2 weeks after grafting (Figure 3A). This example highlights the growth and [18F]FDG avidity of tumors located at the periphery of the thoracic cavity and along the heart great vessels (white arrows). [18F]FDG uptake in tumors was quantified by extracting SUVmax in ROIs drawn over tumors, with the help of CT scans, and shows significant time-dependent increases of their glucose metabolism (Figure 3B). Correlation analyses demonstrated that SUVmax were positively correlated to the time of monitoring with a coefficient of determination R2 of 0.7 (Figure 3C). These data demonstrate the reliability of [18F]FDG-PET scans to monitor the fate of H2052/484 orthotopic tumors. Finally, lung volumes and [18F]FDG avidity, respectively, analyzed by CT and PET, correlate with each other with an R2 of 0.6 supporting the strength of these measurements to study MPM orthotopic tumors development (Figure 4).
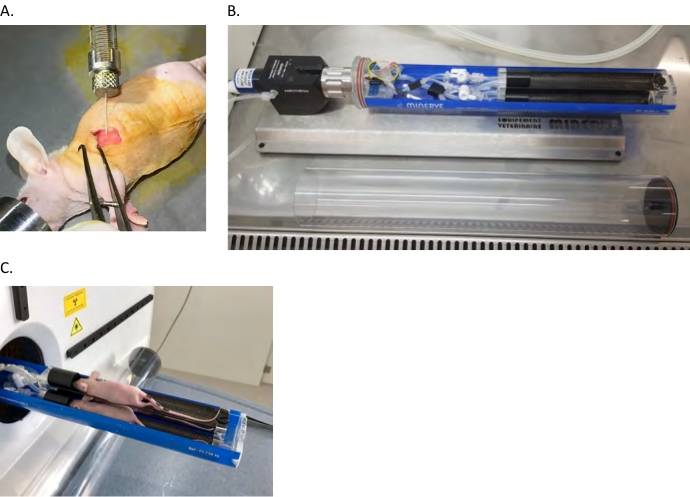
Figure 1: Nude mouse orthotopic xenograft model. (A) Intrapleural (ipl) injection of human MPM cells into the left pleural cavity as described in the protocol section. (B,C) Mice are anesthetized and loaded in the PET/CT bed in a laminar flow hood then transferred to the scanner. Please click here to view a larger version of this figure.
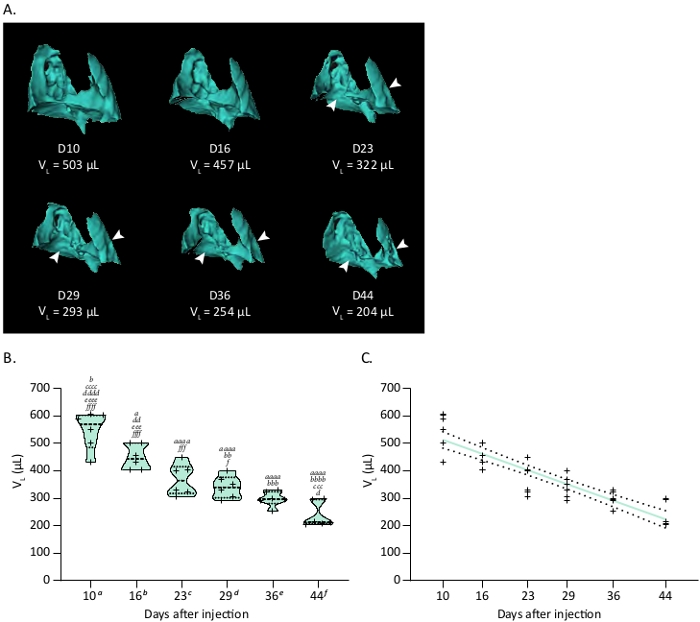
Figure 2: Tumor growth of the orthotopic H2052/484 MPM model monitored by CT. (A) Representative 3D reconstructions of CT scans showing H2052/484 MPM ipl tumors and their effect on the lung volume (Vp) at various time in days after implantation. White arrowheads show location of MPM ipl tumors. (B) Violin plot showing a representative time course of lung volumes (VL), n = 6. One-way ANOVA test with Tukey’s multiple comparisons statistics are indicated. Letters indicate significant differences between models with a, b, c, d, e, f indicating respectively D10, D16, D23, D29, D36 and D44. Corresponding p values: x, p < 0.05; xx, p < 0.01; xxx, p < 0.001; xxxx, p < 0.0001. (C) Correlation between the decrease of lung volume related to ipl MPM development and time after injection. Linear regression is plotted as a thick colored line and related SD as dashed black lines. Graphs and statistical analyses were performed with software. Please click here to view a larger version of this figure.
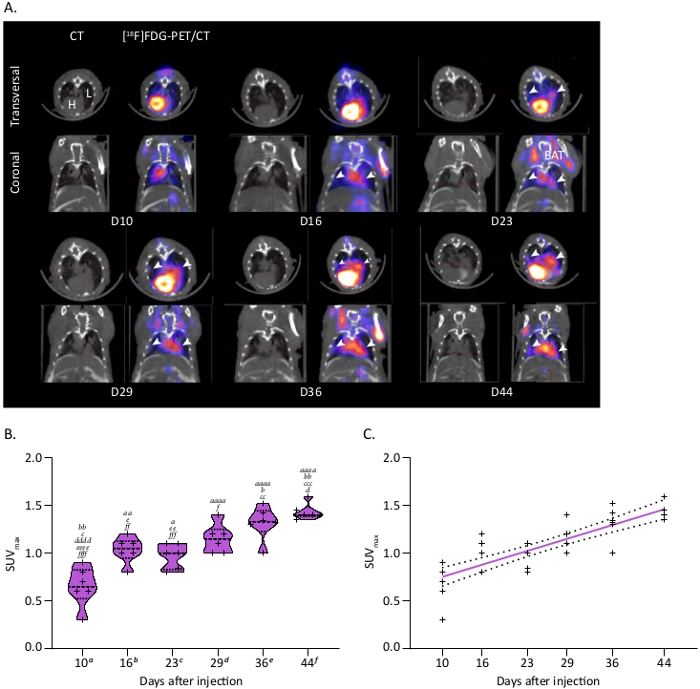
Figure 3: Tumor metabolism of the ipl MPM model followed by [18F]FDG-microPET/CT. (A) Representative PET/CT scans showing MPM ipl tumors. PET/CT images show trans-axial slices of the chest area containing the [18F]FDG-avid tumors, with CT (grey scale) providing anatomical information and PET (calibrated pseudo-color scale) showing the location and intensity of high tumor and organ glucose utilization. Post-injection days are indicated. CT: CT mediastinal window; [18F]FDG-PET/CT: fused image of PET and CT scans. White arrowheads show MPM ipl tumors. L = lung, H = heart, BAT = brown adipose tissue. (B) Violin plot showing a representative time course of SUVmax linked to MPM metabolism, n = 6. One-way ANOVA test with Tukey’s multiple comparisons statistics are indicated. Letters indicate significant differences between models with a, b, c, d, e, f indicating respectively D10, D16, D23, D29, D36 and D44. Corresponding p values: x, p < 0.05; xx, p < 0.01; xxx, p < 0.001; xxxx, p < 0.0001. (C) Correlation between the increase of SUVmax in ipl MPM tumors and time after injection. Linear regression is plotted as a thick colored line and related SD as dashed black lines. Graphs and statistical analyses were performed with software. Please click here to view a larger version of this figure.
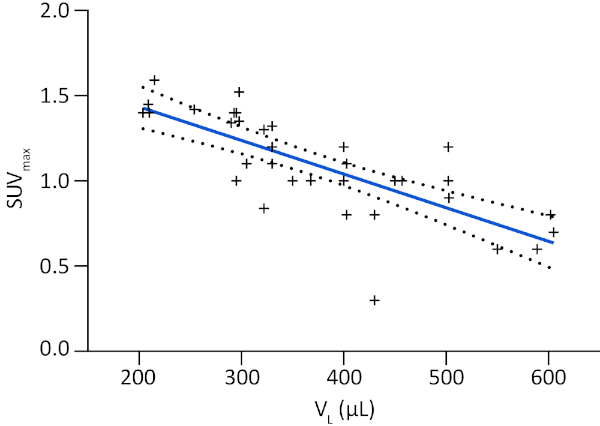
Figure 4: Correlation between MPM development monitored by lung volume and metabolic tumor activity. Correlation between SUVmax and lung volume (VL) displayed as a linear regression plotted as a thick colored line and related SD as dashed black lines. Graphs and statistical analyses were performed with software. Please click here to view a larger version of this figure.
