This procedure has previously been used in three separate experiments. All the experiments were made by different lead investigators who all are co-authors of this article. In all three experiments, great care was taken to adhere to the same procedure as described in this protocol. In all three experiments, secondary lymphedema was induced in one hindlimb while the other hindlimb served as a control. Volumes of the hindlimbs were the primary outcome in all three experiments. Figure 1 illustrates the study design.
All mice underwent micro-computed tomography (µCT) scans in the weeks following surgery to measure the volume of the hindlimbs. The µCT scans were performed on a multimodality pre-clinical scanner (Table of Materials) and the volume of the hindlimbs was measured via the region-of-interest (ROI) function in the associated software as previously described26. The distal tibiofibular joint was located in three-dimensional (3D) axonal images using a method previously described27. The ROI started at the distal tibiofibular joint and included all tissue distal to that point. The Hounsfield range for the analysis was set to -500 to 4000.
All data were analyzed using statistical software (Table of Materials). Sidak's multiple comparison test was used to compare the volume of the induced lymphedema hindlimb, with the control hindlimb. A significant difference between the control hindlimb and lymphedema hindlimb is defined as a P-value <0.05.

Figure 1: Study design and time points for outcome measurements. Please click here to view a larger version of this figure.
Experiment 126 included 32 mice distributed into groups of four. One of the objectives was to study several different doses of radiation and find the most preferable dose, for inducing lasting lymphedema without causing severe morbidity. The group that was given two doses of 10 Gy irradiation included four mice. Figure 2 shows that a consistent state of lymphedema was achieved in all 8 weeks. Table 1 shows that there was a significant difference in volume between the lymphedema hindlimb and control hindlimb in weeks 1, 7, and 8. While a consistent state of induced lymphedema was achieved, there was not a statistically significant difference between the hindlimbs during all 8 weeks. This outcome differs from the two other experiments and could be explained due to the relatively smaller sample size of four mice. Increasing the number of measurements would increase the power of the study and hereby the probability of detecting a difference if a difference exists28.
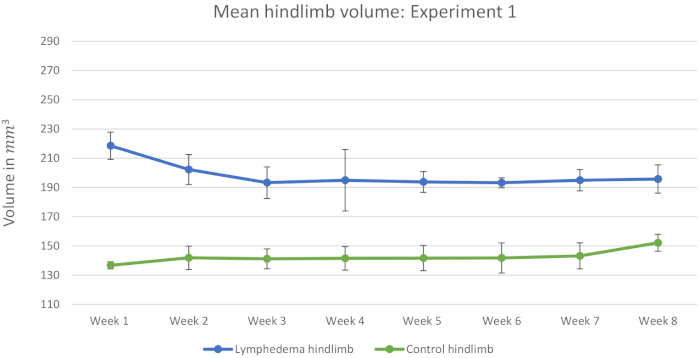
Figure 2: Mean hindlimb volume: Experiment 1. Measurements of 4 mice from the group that was given two doses of 10 Gy irradiation are included in this figure. This graph shows the mean hindlimb volumes in mm3 in the 8 weeks after surgery. All mice received a dose of 10 Gy irradiation pre- and post-surgery. The error bars represent the standard deviation (SD). Please click here to view a larger version of this figure.
| Week | Lymphedema volume in mm3 (n = 4) | Control volume in mm3 (n = 4) | P-value | 95% Confidence interval |
| 1 | 218.53 ± 9.3 | 136.78 ± 2.48 | 0.002 | 53.77−109.73 |
| 2 | 202.25 ± 10.24 | 141.88 ± 8.02 | 0.066 | (-6.53)−127.28 |
| 3 | 193.28 ± 10.80 | 141.20 ± 6.80 | 0.060 | (-3.7)−107.85 |
| 4 | 194.95 ± 21.05 | 141.50 ± 8.03 | 0.224 | (-41.85)−148.75 |
| 5 | 193.75 ± 7.07 | 141.70 ± 8.60 | 0.051 | (-0.27)−104.37 |
| 6 | 193.23 ± 3.42 | 141.78 ± 10.29 | 0.054 | (-1.56)−104.46 |
| 7 | 194.95 ± 7.26 | 143.23 ± 8.90 | 0.050 | 0.17−103.28 |
| 8 | 195.8 ± 9.65 | 152.18 ± 5.81 | 0.009 | 19.88−67.38 |
Table 1: Sidak's multiple comparisons test: Experiment 1. This table shows the statistical comparison between the mean volumes of induced lymphedema hindlimbs and control hindlimbs during the 8 weeks after surgery. All mice received a dose of 10 Gy irradiation pre- and post-surgery. Values are presented as: mean ± SD in mm3. P-value < 0.05 is considered as a significant difference between the control hindlimb and lymphedema hindlimb. n (number of observations) = 4.
Experiment 2 included 45 mice. 15 mice served as controls and were given saline injections. The controls are used as representative results as we assume that the saline injections had no effect on the volume of induced lymphedema. Figure 3 shows that the lymphedema was less stable than in experiment 1. Additionally, the volume of the control hindlimbs increased during the 8 weeks. This decreases the relative difference presented in Table 2. It has been speculated that the mice use their non-operated hindlimb more, in the weeks following surgery, and that this leads to hypertrophy and increase in limb volume of the non-operated hindlimb. Most importantly, Table 3 shows that there is statistically significant difference between the lymphedema hindlimb and the control hindlimb during all 8 weeks after surgery. The higher number of mice proves that this procedure can induce statistically significant lymphedema for at least 8 weeks.
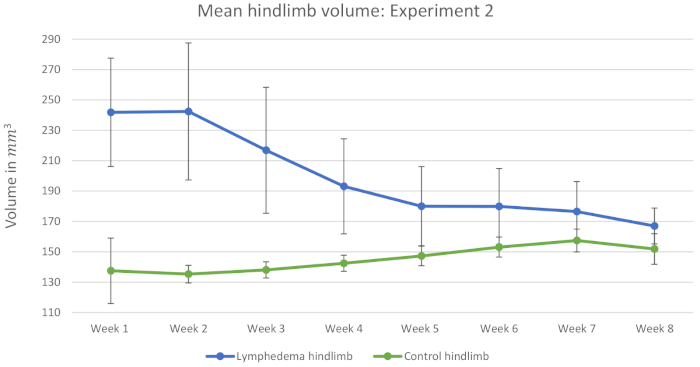
Figure 3: Mean hindlimb volume: Experiment 2. Measurements of 15 mice from the control group are included in this figure. This graph shows the mean hindlimb volumes in mm3 in the 8 weeks after surgery. All mice received a dose of 10 Gy irradiation pre- and post-surgery. The error bars represent SD. Please click here to view a larger version of this figure.
| Experiment 1 | Experiment 2 | Experiment 3 | Experiment 1, 2 and 3 combined | |||||
| Week | Absolute difference (mm3) | Relative difference (%) | Absolute difference (mm3) | Relative difference (%) | Absolute difference (mm3) | Relative difference (%) | Absolute difference (mm3) | Relative difference (%) |
| 1 | 81.75 ± 7.20 | 0.60 ± 0.04 | 104.34 ± 25.96 | 0.76 ± 0.23 | 85.20 ± 35.05 | 0.64 ± 0.27 | 94.02 ± 29.57 | 0.69 ± 0.24 |
| 2 | 60.38 ± 17.21 | 0.43 ± 0.14 | 107.12 ± 44.33 | 0.79 ± 0.33 | 85.63 ± 37.94 | 0.63 ± 0.29 | 92.77 ± 41.68 | 0.68 ± 0.31 |
| 3 | 52.08 ± 14.35 | 0.37 ± 0.11 | 78.77 ± 39.45 | 0.57 ± 0.28 | 74.67 ± 49.57 | 0.54 ± 0.38 | 73.74 ± 41.51 | 0.53 ± 0.31 |
| 4 | 53.45 ± 24.51 | 0.38 ± 0.19 | 50.67 ± 29.94 | 0.36 ± 0.21 | 50.62 ± 16.35 | 0.37 ± 0.11 | 51.01 ± 24.03 | 0.37 ± 0.17 |
| 5 | 52.05 ± 13.46 | 0.37 ± 0.11 | 32.74 ± 24.66 | 0.22 ± 0.17 | 42.67 ± 11.81 | 0.31 ± 0.07 | 39.08 ± 20.02 | 0.27 ± 0.14 |
| 6 | 51.45 ± 13.63 | 0.36 ± 0.11 | 26.80 ± 22.35 | 0.18 ± 0.14 | 32.86 ± 10.90 | 0.22 ± 0.08 | 32.32 ± 18.96 | 0.21 ± 0.13 |
| 7 | 51.73 ± 13.26 | 0.36 ± 0.11 | 19.04 ± 17.22 | 0.12 ± 0.11 | – | – | 25.92 ± 21.15 | 0.17 ± 0.15 |
| 8 | 43.63 ± 6.11 | 0.29 ± 0.04 | 15.15 ± 11.70 | 0.10 ± 0.08 | – | – | 21.15 ± 15.96 | 0.14 ± 0.10 |
Table 2: Absolute and relative difference. This table shows the absolute difference in volume between lymphedema- and control hindlimbs ± SD in mm3 and the relative difference ± SD in percent.
| Week | Lymphedema volume in mm3 (n = 15) | Control volume in mm3 (n = 15) |
P-value | 95% Confidence interval |
| 1 | 241.82 ± 35.69 | 137.48 ± 21.54 | <0.001 | 82.21−126.47 |
| 2 | 242.41 ± 45.13 | 135.29 ± 5.81 | <0.001 | 69.33−144.89 |
| 3 | 216.85 ± 41.47 | 138.08 ± 5.31 | <0.001 | 45.15−112.39 |
| 4 | 193.10 ± 31.27 | 142.43 ± 5.29 | <0.001 | 25.15−76.18 |
| 5 | 180.03 ± 26.03 | 147.29 ± 6.45 | 0.002 | 11.72−53.76 |
| 6 | 179.89 ± 25.00 | 153.09 ± 6.56 | 0.004 | 7.74−45.85 |
| 7 | 176.45 ± 19.77 | 157.41 ± 7.49 | 0.008 | 4.35−33.71 |
| 8 | 166.97 ± 11.8 | 151.82 ± 10.07 | 0.002 | 5.18−25.12 |
Table 3: Sidak's multiple comparisons test: Experiment 2. This table shows the statistical comparison between the mean volumes of induced lymphedema hindlimbs and control hindlimbs in the 8 weeks after surgery. All mice received a dose of 10 Gy irradiation pre- and post-surgery. Values are presented as: mean ± SD in mm3. P-value < 0.05 is considered as a significant difference between the control hindlimb and lymphedema hindlimb. n (number of observations) = 15.
Experiment 3 included 36 mice. 12 mice served as controls and were given saline injections. The controls are used as representative outcome as we assume that the saline injections had no effect on the volume of induced lymphedema. In this experiment the hindlimb volume of the mice were measured for 6 weeks instead of 8. The experiment only lasted 6 weeks due to logistical difficulties when the experiment was performed. Figure 4 shows a more consistent lymphedema than experiment 2. Table 4 shows that there is statistically significant lymphedema in the 6 weeks after surgery.
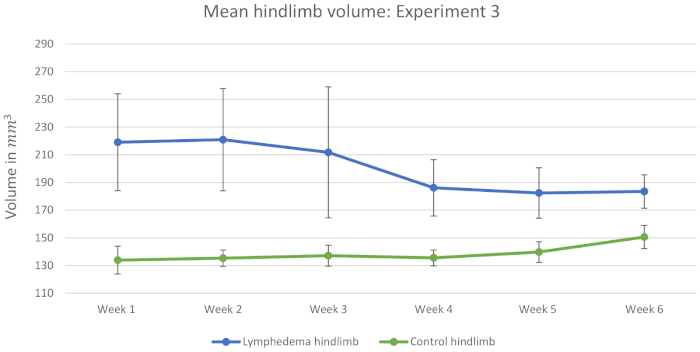
Figure 4: Mean hindlimb volume: Experiment 3. Measurements of 12 mice from the control group are included in this figure. This graph shows the mean hindlimb volumes in mm3 in the 6 weeks after surgery. All mice received a dose of 10 Gy irradiation pre- and post-surgery. The error bars represent SD. Please click here to view a larger version of this figure.
| Week | Lymphedema volume in mm3 (n = 12) | Control volume in mm3 (n = 12) | P-value | 95% Confidence interval |
| 1 | 219.06 ± 35.00 | 133.86 ± 10.02 | <0.001 | 51.66−118.74 |
| 2 | 220.90 ± 36.98 | 135.27 ± 5.89 | <0.001 | 49.33−121.94 |
| 3 | 211.74 ± 47.30 | 137.07 ± 7.56 | 0.002 | 27.24−122.11 |
| 4 | 186.09 ± 20.36 | 135.47 ± 5.70 | <0.001 | 34.98−66.27 |
| 5 | 182.35 ± 18.25 | 139.68 ± 7.45 | <0.001 | 31.37−53.98 |
| 6 | 183.44 ± 12.11 | 150.58 ± 8.37 | <0.001 | 22.42−43.29 |
Table 4: Sidak's multiple comparisons test: Experiment 3. This table shows the statistical comparison between the mean volumes of induced lymphedema hindlimbs and control hindlimbs in the 6 weeks after surgery. All mice received a dose of 10 Gy irradiation pre- and post-surgery. Values are presented as: mean ± SD in mm3. P-value < 0.05 is considered as a significant difference between the control hindlimb and lymphedema hindlimb. n (number of observations) = 12.
Figure 5 and Table 5 shows the mean hindlimb volume of all three experiments combined. Table 5 shows that the use of this procedure results in statistically significant lymphedema lasting at least 8 weeks. Data from the first 6 weeks, are the combined measurements of 31 mice from experiments 1, 2 and 3. In week 7−8 we only had data from experiments 1 and 2 resulting in combined measurements from 19 mice.
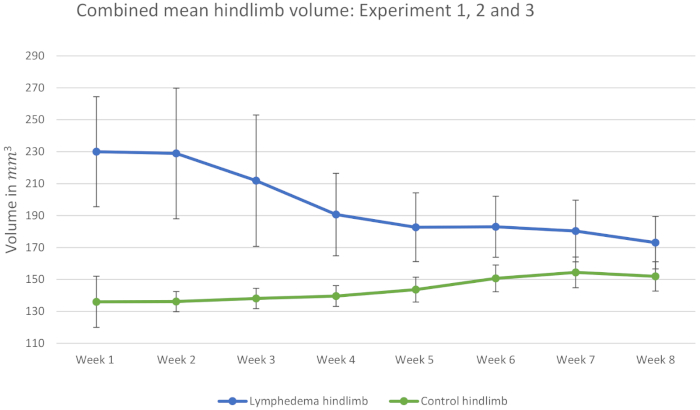
Figure 5: Combined mean hindlimb volume: Experiment 1, 2 and 3. Thirty-one mice included in the first 6 weeks after surgery and 19 mice included in the following 2 weeks. This graph shows the mean hindlimb volumes in mm3 in the 8 weeks after surgery. All mice received a dose of 10 Gy irradiation pre- and post-surgery. The error bars represent SD. Please click here to view a larger version of this figure.
| Week | Lymphedema volume in mm3 (Week 1−6 n = 31) (Week 7−8 n = 19) |
Control volume in mm3 (Week 1−6 n = 31) (Week 7−8 n = 19) |
P-value | 95% Confidence interval |
| 1 | 230.00 ± 34.46 | 135.99 ± 16.03 | <0.001 | 78.19−109.84 |
| 2 | 228.90 ± 40.91 | 136.13 ± 6.32 | <0.001 | 70.47−115.07 |
| 3 | 211.83 ± 41.15 | 138.09 ± 6.36 | <0.001 | 51.53−95.95 |
| 4 | 190.63 ± 25.81 | 139.62 ± 6.54 | <0.001 | 38.15−63.87 |
| 5 | 182.70 ± 21.52 | 143.62 ± 7.79 | <0.001 | 28.36−49.79 |
| 6 | 182.98 ± 19.11 | 150.66 ± 8.36 | <0.001 | 22.18−42.47 |
| 7 | 180.34 ± 19.31 | 154.43 ± 9.60 | <0.001 | 11.61−40.22 |
| 8 | 173.04 ± 16.42 | 151.89 ± 9.19 | <0.001 | 10.35−31.94 |
Table 5: Sidak's multiple comparisons test: Experiment 1, 2 and 3 combined. This table shows the statistical comparison between the mean volumes of induced lymphedema hindlimbs and control hindlimbs of 31 mice in the first 6 weeks after surgery and 19 mice in the following 2 weeks. All mice received a dose of 10 Gy irradiation pre- and post-surgery. Values are presented as: mean ± SD in mm3. P-value < 0.05 is considered as a significant difference between the control hindlimb and lymphedema hindlimb. n (number of observations) = 31.
