When interpreting the results, it is important to remember that lower threshold estimates indicate greater sensory acuity. The use of a forced choice procedure helps separates criterion response bias (i.e., a willingness to say yes) from underlying sensitivity of the system. A lower threshold indicates an individual can perceive a lighter stimulus than those with a higher threshold estimate. Higher threshold estimates indicate decreased sensory acuity. A higher threshold estimate indicates an individual requires a larger input to cognitively perceive the stimulus. Higher threshold estimates could be due to difficulty in cognitively completing the task16,21 or due to peripheral damage associated with advancing age or disorder to the cutaneous surface of the tongue or peripheral nerves22.
Data is still being collected to further develop normative data from a sample of nominally healthy adults. However, a sample of data on individual differences in oral somatosensory function was recently published7. Combining previously published data with additional data, a total of 111 healthy participants (34M:77F; mean 32.1 years, range 18 to 68 years) completed at least one portion of the detection and/or discrimination threshold estimate protocol described here.
| Detection | Discrimination | |||
| (n= 51) | (n= 107) | |||
| Location | M (SD) | Range | M (SD) | Range |
| Midline Tongue | 0.0157 (0.022) | 0.008-0.16 | 0.600 (1.812) | 0.02-15 |
Table 1: Detection and discrimination threshold estimates for pressure point sensitivity on midline tongue. The geometric mean, standard deviation and range are provided from our representative sample. Fifty one participants completed detection threshold estimate testing (10M:41F, mean 37.1 years). A total of 107 participants completed discrimination threshold estimate testing (31M: 76F, mean 31.9 years).
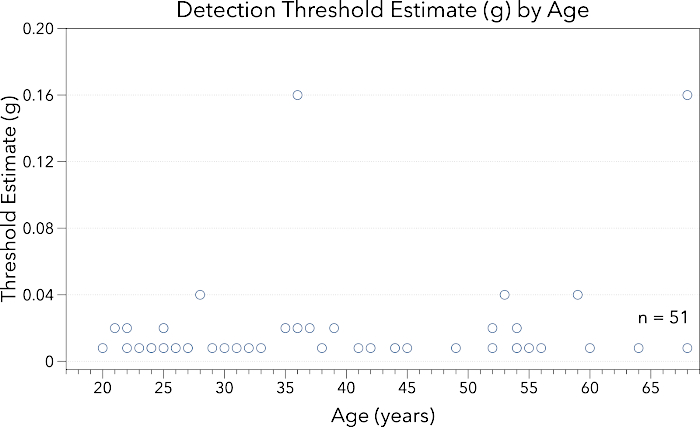
Figure 1: This figure presents data for midline lingual point pressure detection threshold estimate (g) by participant age (years). Note the y-axis ranges from 0.0 – 0.25 g. Participants across this healthy age span demonstrated low thresholds for point-pressure detection. Please click here to view a larger version of this figure.
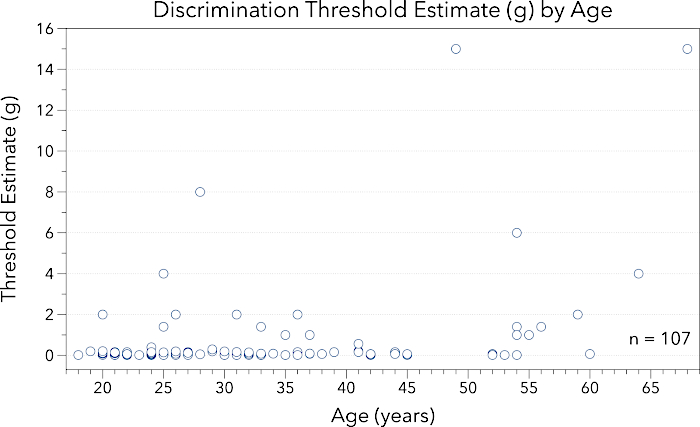
Figure 2: This figure provides data for midline lingual point pressure discrimination threshold estimate (g) by participant age (years). Note the y-axis ranges from 0.0 – 16.0 g. Participants across this healthy age span demonstrated increased variability in discrimination threshold estimates as compared to detection threshold estimates. Please click here to view a larger version of this figure.
Supplementary Materials
Two potential options for setting up data recording sheets are available in the Supplementary Files. Data can easily be recorded and visualized using a one page data collection sheet (Supplementary files 1 & 2). On this sheet, both detection and discrimination data can be recorded in their respective sections. The list of Von Frey Hair monofilament targets in grams (g) and the color of the pen are included on the left hand side. An asterisk (*) has been placed next to the 1.000 g target in the 'Detection' section to remind testers of the starting point for testing using this protocol. The trial numbers are listed across the bottom to easily identify the total number of trials needed. The authors suggest following the key listed on the bottom right to mark correct and incorrect participant responses. A second data recording option is provided in Supplementary Files 3 & 4. The series number is noted in the column marked #. The target or test stimuli is recorded in grams in the column labeled 'Target (g)'. The next two columns are labeled 'Trial 1' and 'Trial 2' to indicate in which the trial the tester should deliver the test stimuli. This pattern was created using a random number generator. Experimenters will present the test stimuli in the trial with the "X" in it. For example, in the first series, the target stimuli would be delivered in the second trial because the "X" is under the Trial 2 heading. Finally, in the last column, the experimenter can record the participant's response as correct (Y) or incorrect (N). This column can also be used to note the number of presentations of that target to aide in identifying the stopping point.
Supplementary File 1. Please click here to view this file.
Supplementary File 2. Please click here to view this file.
Supplementary File 3. Please click here to view this file.
Supplementary File 4. Please click here to view this file.
