The mean and standard deviation of the spatial-temporal, kinematics, and kinetic gait parameters are given in Table 2. MVIC data for all 30 participants are summarized in Table 3. A typical set of data for the left and right side of one participant showing graphical representation of gait parameters is provided in Figure 4 and Figure 5, respectively.
The data presented are representative of the results obtained across all participants, and are consistent with textbook reference results obtained for gait and isometric strength testing15.
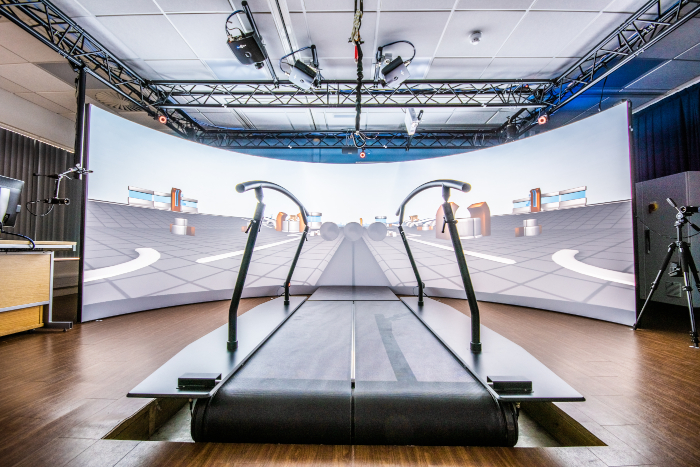
Figure 1: Gait analysis system. The GRAIL system is used to measure gait parameters. This system consists of a split-belt instrumented treadmill, 160° semi-cylindrical projection screen, force sensors, video cameras and optical infrared system. Please click here to view a larger version of this figure.
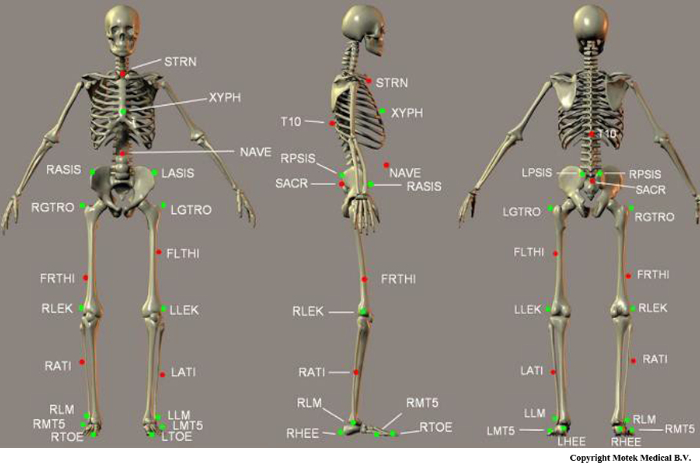
Figure 2: Diagram of markers used in Human Body Model (HBM). This figure shows the exact placements of all markers in the HBM lower body model. Special attention should be paid to the placement of the markers printed in green (bold in Table 1); these are used during initialization to define the biomechanical skeleton. This figure is adapted from the HBM Reference Manual8. Please click here to view a larger version of this figure.

Figure 3: The muscle strength testing equipment (multimodal dynamometer) used to measure participants lower limb muscle strength. This system is used to measure the participants' muscle strength based on Maximum Voluntary Isometric Contraction (MVIC). Please click here to view a larger version of this figure.
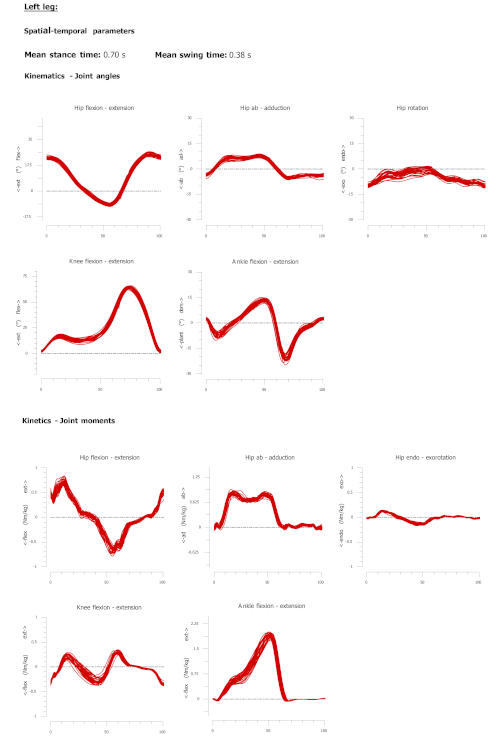
Figure 4: A sample report produced from offline analysis of the gait assessment using the proposed technique. Spatial temporal data and kinematic and kinetic gait cycle for the left side of one participant. Each line represents one gait cycle. The Y-axis represents the joint angles in degrees for the kinematic plots and joint moment in newton meter per kilogram for the kinetic plots. Red lines represent left side gait parameters. Please click here to view a larger version of this figure.
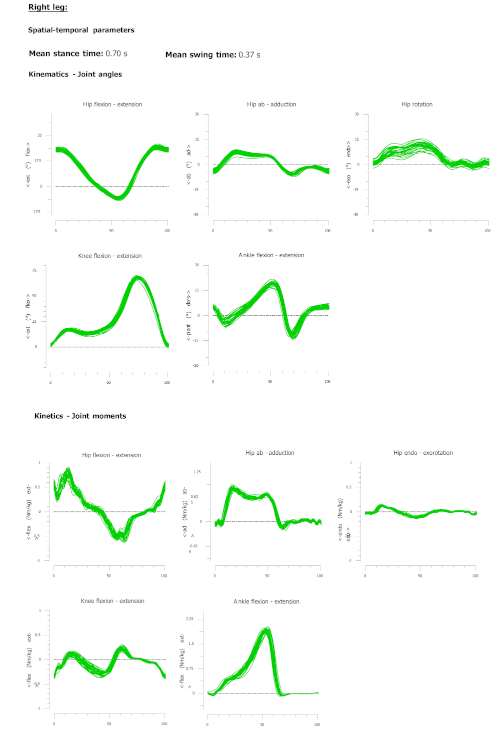
Figure 5: A sample report produced from offline analysis of the gait assessment using the proposed technique. Spatial temporal data and kinematic and kinetic gait cycle for the right side of one participant. Each line represents one gait cycle. The Y-axis represents the joint angles in degrees for the kinematic plots, and joint moment in newton meter per kilogram for the kinetic plots. The Green lines represent right side gait parameters. Please click here to view a larger version of this figure.
| Label | Anatomical location | Description |
| T10 | T10 | On the 10th thoracic vertebrae |
| SACR | Sacrum bone | On the sacral bone |
| NAVE | Navel | On the navel |
| XYPH | Xiphoid process | Xiphiod procces of the sternum |
| STRN | Sternum | On the jugular notch of the sternum |
| LASIS | Pelvic bone left front | Left anterior superior iliac spine |
| RASIS | Pelvic bone right front | Right anterior superior iliac spine |
| LPSIS | Pelvic bone left back | Left posterior superior iliac spine |
| RPSIS | Pelvic bone right back | Right posterior superior iliac spine |
| LGTRO | Left greater trochanter of the femur | On the center of the left greater trochanter |
| FLTHI | Left thigh | On 1/3 on the line between the LGTRO and LLEK |
| LLEK | Left lateral epicondyle of the knee | On the lateral side of the joint axis |
| LATI | Left anterior of the tibia | On 2/3 on the line between the LLEK and LLM |
| LLM | Left lateral malleolus of the ankle | The center of left lateral malleolus |
| LHEE | Left heel | Center of the heel at the same height as the toe |
| LTOE | Left toe | Tip of big toe |
| LMT5 | Left 5th meta tarsal | Caput of the 5th meta tarsal bone, on joint line midfoot/toes |
| RGTRO | Right greater trochanter of the femur | On the center of the right greater trochanter |
| FRTHI | Right thigh | On 2/3 on the line between the RGTRO and RLEK |
| RLEK | Right lateral epicondyle of the knee | On the lateral side of the joint axis |
| RATI | Right anterior of tibia | On 1/3 on the line between the RLEK and RLM |
| RLM | Right lateral malleolus of the ankle | The center of right lateral malleolus |
| RHEE | Right heel | Center of the heel at the same height as toe |
| RTOE | Right toe | Tip of big toe |
| RMT5 | Right 5th meta tarsal | Caput of the 5th meta tarsal bone, on joint line midfoot/toes |
Table 1: Markers used in the Human Body Model (HBM). This table shows the exact placements of all markers in the HBM lower body model. Special attention should be paid to the placement of the markers written in bold; these are used during initialization to define the biomechanical skeleton. This table is adapted from the HBM Reference Manual8.
| Variable name | Side | Mean | Standard Deviation |
| Spatial temporal | |||
| Walking speed (m/s) | 1.37 | 0.22 | |
| Step length (m) | Left | 0.72 | 0.07 |
| Right | 0.73 | 0.07 | |
| Stride time (s) | Left | 1.07 | 0.10 |
| Right | 1.07 | 0.10 | |
| Stance time (s) | Left | 0.70 | 0.08 |
| Right | 0.70 | 0.08 | |
| Swing time (s) | Left | 0.37 | 0.03 |
| Right | 0.37 | 0.03 | |
| Kinematic | |||
| Hip Flex (deg) | Left | 30.05 | 9.08 |
| Right | 29.92 | 8.79 | |
| Hip Ext (deg) | Left | -13.26 | 7.75 |
| Right | -13.36 | 7.68 | |
| Hip Abd (deg) | Left | -7.27 | 3.00 |
| Right | -7.72 | 3.17 | |
| Hip Add (deg) | Left | 8.66 | 4.22 |
| Right | 7.81 | 3.72 | |
| Hip Int Rot (deg) | Left | 5.38 | 6.95 |
| Right | 6.82 | 6.42 | |
| Hip Ext Rot (deg) | Left | -9.04 | 7.03 |
| Right | -5.77 | 5.97 | |
| Knee Flex (deg) | Left | 67.46 | 5.16 |
| Right | 68.47 | 4.75 | |
| Knee Ext (deg) | Left | -0.43 | 2.26 |
| Right | -0.29 | 2.01 | |
| Ankle Flex (deg) | Left | -17.20 | 6.94 |
| Right | -14.91 | 6.47 | |
| Ankle Ext (deg) | Left | 18.13 | 5.92 |
| Right | 19.36 | 6.54 | |
| Kinetic | |||
| Peak Hip Ext (Nm/kg) | Left | 0.82 | 0.21 |
| Right | 0.80 | 0.24 | |
| Peak Hip Abd (Nm/kg) | Left | 0.91 | 0.15 |
| Right | 0.92 | 0.11 | |
| Peak Hip Int Rot (Nm/kg) | Left | 0.26 | 0.13 |
| Right | 0.26 | 0.14 | |
| Peak Knee Ext (Nm/kg) | Left | 0.38 | 0.06 |
| Right | 0.39 | 0.06 | |
| Peak Ankle Flex (Nm/kg) | Left | 1.85 | 0.21 |
| Right | 1.86 | 0.22 |
Table 2: The mean and standard deviation of the spatial-temporal, kinematics, kinetic gait parameters for the 30 participants. Gait parameters are reported for the left and the right side separately.
| Variable name | Side | Mean | Standard Deviation |
| Knee Ext | Left | 527.17 | 136.42 |
| Right | 550.60 | 132.55 | |
| Knee Flex | Left | 191.60 | 38.53 |
| Right | 203.87 | 47.67 |
Table 3: The mean and standard deviation of the Maximum Voluntary Isometric Contraction (MVIC) for knee joint using the muscle strength testing equipment for the 30 participants.
Supplementary File 1: Matlab coding file. Please click here to view this file (Right click to download).
