Construct fabrication is considered unsuccessful if rats develop an infection or do not survive surgical anesthesia. Previous research has indicated these constructs require approximately three months to revascularize and reinnervate2,3,17,36. Following the three-month recovery period, construct testing can be pursued to examine viability. Surgical exposure of the constructs after three months will reveal revascularized muscle and skin if successful (Figure 3). At times, the free muscle and dermal grafts can consist solely of scar tissue, and/or the nerve will not be attached to the construct; these findings indicate an unsuccessful attempt. However, if successful, gentle squeezing of the common peroneal nerve with forceps proximal to the construct will result in visible muscle contraction (Video 1). Histological analysis of constructs should demonstrate viable skin, nerve, and muscle (Figure 4). Immunostaining will also reveal motor and sensory nerve reinnervation to their neuromuscular junctions and sensory end organs, respectively (Figure 5). If the common peroneal nerve does not reinnervate those tissues, immunostaining will not demonstrate any individual nerve fibers within the construct with the exception of the implanted nerve itself.
Electrophysiologic testing can be performed on these constructs in vivo (Figure 6); previous research has been conducted at 3 and 9 months following C-RPNI fabrication36 (Table 1). Following maximal stimulation with a hook electrode at the proximal common peroneal nerve just distal to its takeoff from the sciatic nerve, compound muscle action potentials (CMAPs) can be measured at the muscle component with visible muscle contraction. The type of electrode used at the muscle can vary according to preference, but epimysial patch, epimysial pad, and bipolar probe electrodes have been used successfully in this research. The average CMAP amplitude recorded at the muscle was 8.7 ± 1.6 mV at 3 months and 10.2 ± 2.1 mV at 9 months. The average conduction velocity was 10 ± 1.2 m/s at 3 months and 9.5 ± 0.6 m/s at 9 months. In comparison, CMAPs generated by physiologic EDL muscle typically range from 10-18 mV37. Following stimulation at the dermal component of the C-RPNI, compound sensory nerve action potentials (CSNAPs) were produced at the proximal common peroneal nerve, with average CSNAP amplitude measuring 113.7 ± 35.1 µV at 3 months and 142.9 ± 63.7 µV at 9 months. Figure 7 illustrates single and summation CMAP and CSNAP signals obtained during electrophysiologic testing in a graphical format.
The C-RPNI serves to amplify a nerve's inherent microvolt signal, and previous research has demonstrated sufficient amplification from the microvolt to millivolt level38. Therefore, if a construct does not provide that level of amplification, it is not considered successful. If either the dermal, muscle, or both components of the C-RPNI fail, testing would result in recordings that mimic the stimulation signal utilized. For the muscle component specifically, a suboptimal result (but one that is still considered operational) would be one that has CMAP amplitude and conduction velocity in the range that falls between the signal stimulation value and that of physiologic EDL muscle. Additionally, these signals can become attenuated and lack the characteristic CMAP waveform (Figure 8A). Suboptimal results at the level of the dermal component can occur but are difficult to quantify given that rats cannot express the quality of sensation they experience. These suboptimal results usually involve dampening of the waveform with significant background noise (Figure 8B). However, if there is significant scarring or callusing of the skin graft, or minimal graft survived, no CSNAPs will be appreciated at the proximal common peroneal nerve regardless of stimulation value.
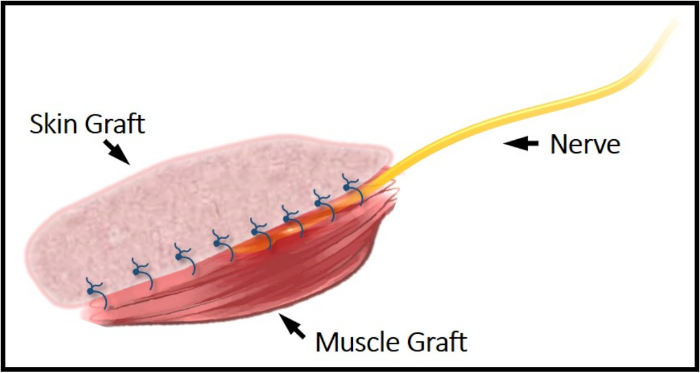
Figure 1: Illustrative schematic of the C-RPNI construct. The common peroneal nerve can be seen secured between the top dermal layer and bottom muscle layer. This construct is secured to the femur periosteum proximally and distally via EDL's tendinous junctions. Please click here to view a larger version of this figure.
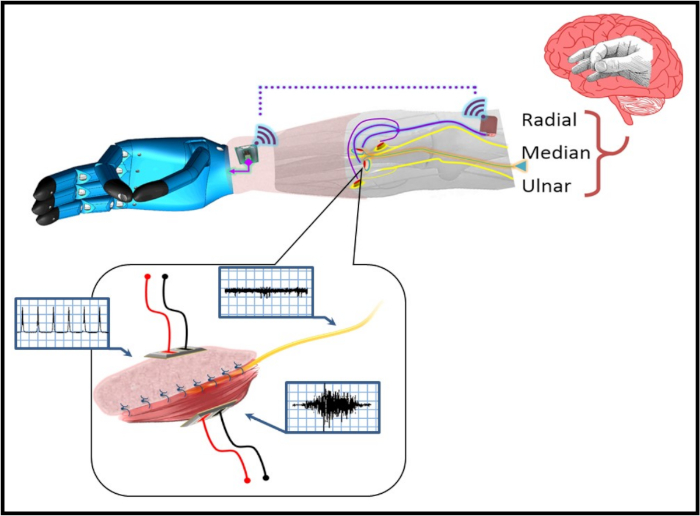
Figure 2: A pictorial representation of the C-RPNI in a patient with a trans-radial amputation. The user forms a desired motor intention at the cerebral level (e.g., pincer grasp), which is transmitted as an efferent motor signal to the C-RPNI via the implanted peripheral nerve. This signal generates a compound muscle action potential (CMAP) at the muscle component, which is recorded by implanted electrodes and recognized by the prosthetic device, generating the desired motion. Sensors on the device's fingertips recognize the amount of pressure generated, and relay that information to an electrode implanted in the dermal component of the C-RPNI. These signals activate the corresponding sensory end organs, generating an afferent compound sensory nerve action potential (CSNAP) transmitted through the peripheral nerve to the sensory cortex. An example signal generated at each component is pictured within the blue boxes pictured next to each component. Please click here to view a larger version of this figure.
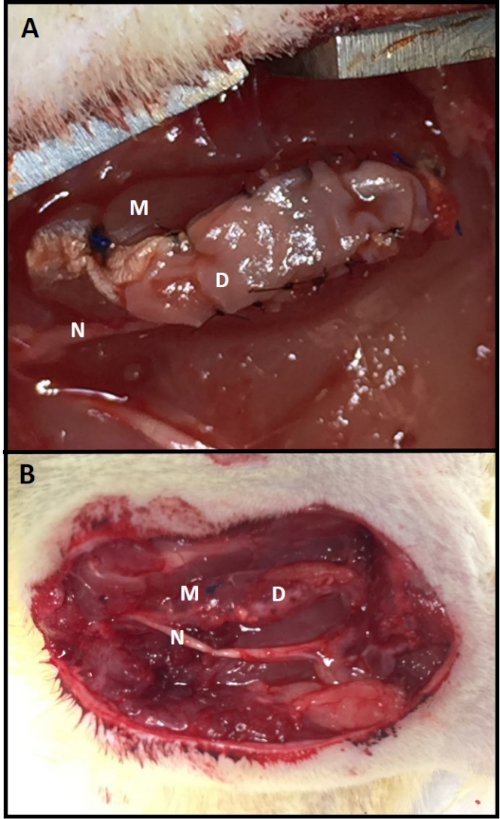
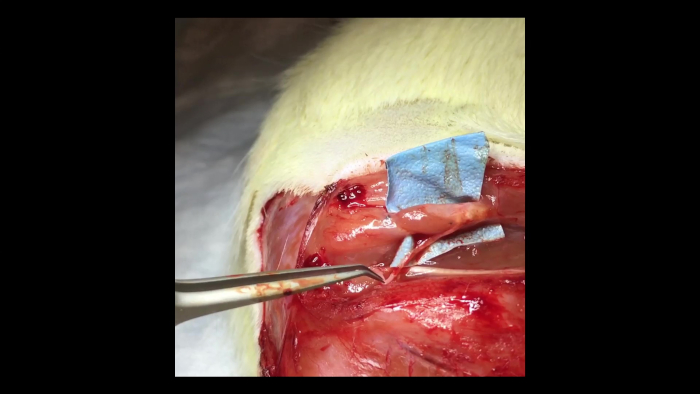
Figure 3: C-RPNI in vivo. (A) A C-RPNI immediately following fabrication and at (B) 3 months post-construction at time of electrophysiologic testing. The muscle component is the deep layer of the construct and the dermal, the superficial. Muscle tissue is marked by (M), dermis (D), and common peroneal nerve (N). Please click here to view a larger version of this figure.
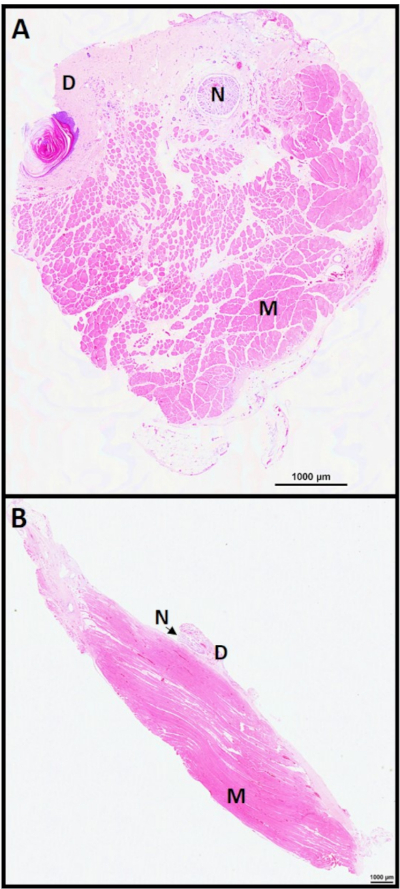
Figure 4: C-RPNI histology 6 months. C-RPNI H&E at 6 months in (A) cross-section and (B) longitudinal section. Muscle noted by (M), dermis (D), and nerve (N). Please click here to view a larger version of this figure.
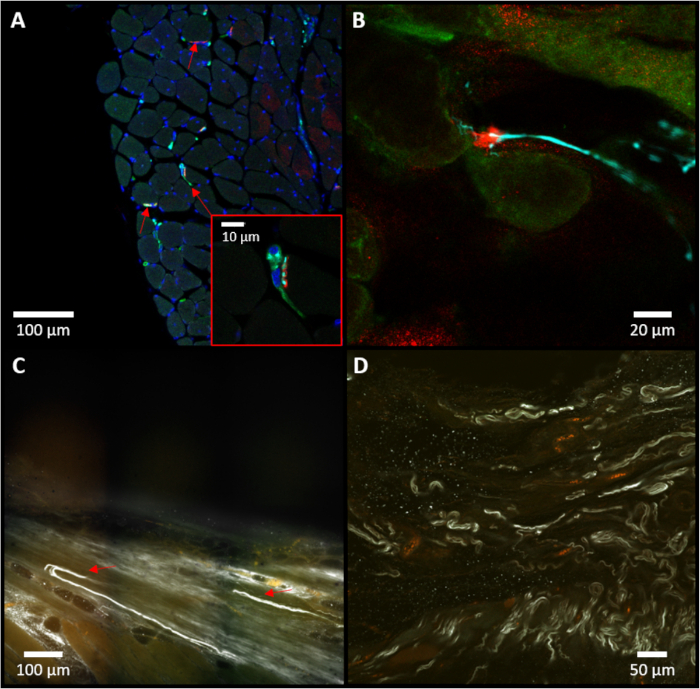
Figure 5: Immunostaining of the C-RPNI. (A) Representative example of a cross-section of muscle tissue, with red arrows identifying neuromuscular junctions. A higher magnification of the central neuro-muscular junction (NMJ) is pictured at the bottom-right. (B) Close-up of a neuromuscular junction noted in the sample. For (A) and (B), red staining (alpha-bungarotoxin) indicates presence of cholinergic receptors in muscle tissue; blue (neurofilament 200) specifies presence of neurofilaments within neuronal tissue; and green (choline acetyltransferase) notes specifically motor neuron presence. (C) Representative example of an iDISCO image focusing on the dermal junction, with red arrows marking sensory neurons (white) entering the dermis. (D) On-lay view of iDISCO demonstrating multiple sensory neurons (white, neurofilament 200). Please click here to view a larger version of this figure.
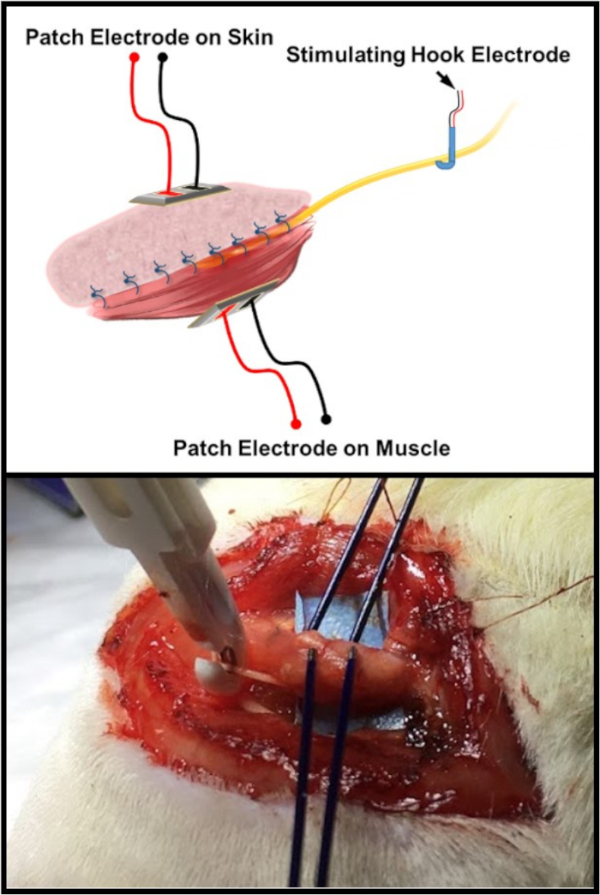
Figure 6: Electrophysiologic testing schematic. The top image is an illustration of the standard electrode arrangement for testing the C-RPNI constructs. There is a patch and/or probe electrode placed on both the muscle and dermal components of the C-RPNI, with a double hook electrode placed at the common peroneal nerve proximally. The bottom image is an in vivo example of the testing arrangement on a rat subject. Please click here to view a larger version of this figure.
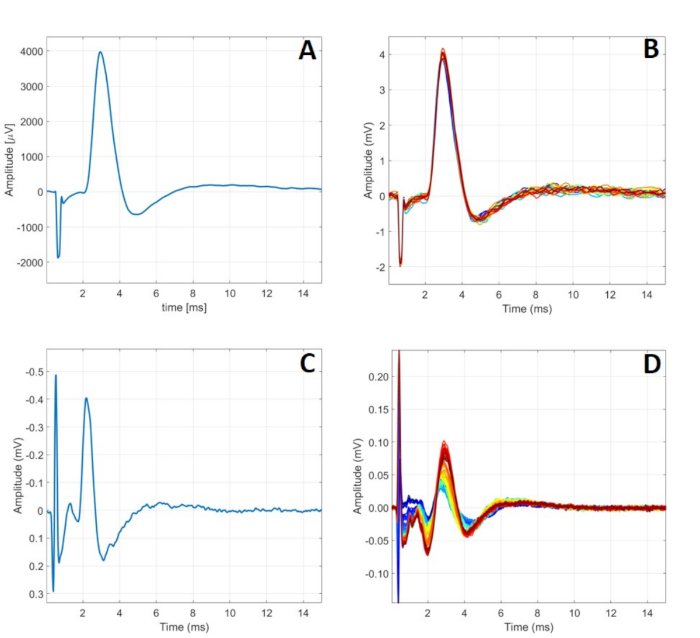
Figure 7: Typical C-RPNI electrophysiologic signaling. (A) A single CMAP signal recorded at the muscle component following a 5.00 mA signal applied to the CP nerve. (B) 24 CMAPs generated by 5.00 mA stimulation at the nerve. (C) A single CSNAP signal recorded from the proximal CP nerve following dermal component stimulation at 900 µA. (D) A series of CSNAPs recorded from the proximal CP nerve following increasing stimulation at the dermal component from 500 µA to 1000 µA. Please click here to view a larger version of this figure.
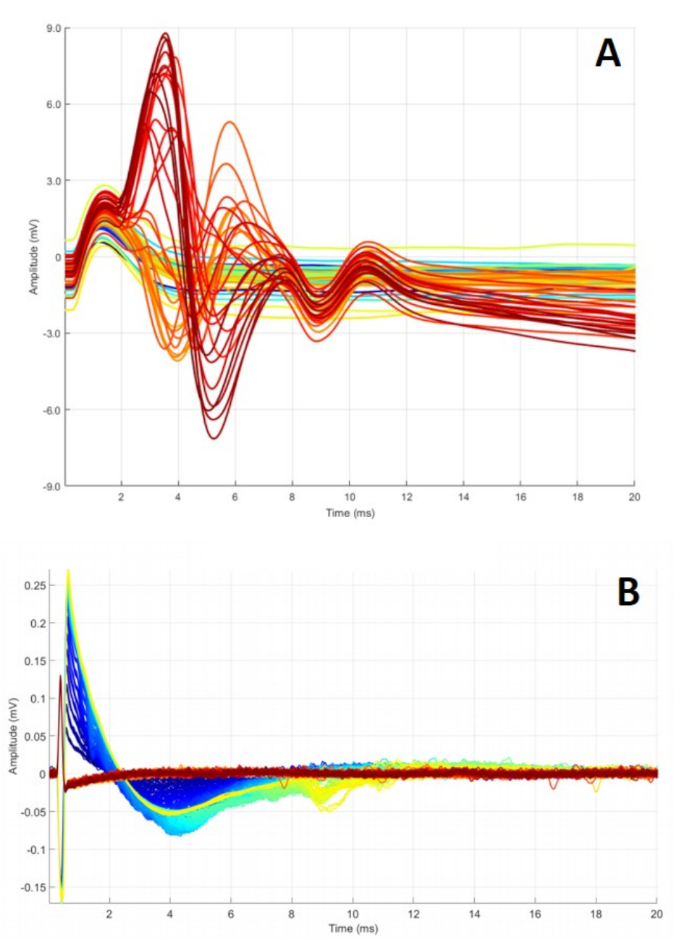
Figure 8: Abnormal C-RPNI signaling. (A) A series of CMAPs obtained while ramping CP nerve stimulation from 0.2 to 4 mA. Waveforms peak at different points and fail to return to baseline, possibly indicating defective electrodes or inadequate overall construct function. (B) Summation of CSNAPs obtained while stimulating dermal component, ramping 0.1 to 5 mA. These findings can occur for a multitude of reasons, including malfunctioning electrode(s), dermal graft scarring, and/or nerve damage. Please click here to view a larger version of this figure.
| 3 Month Data | CMAP Data (Stimulate CP nerve and record from muscle graft) | CSNAP Data (Stimulate skin graft and record from CP nerve) | |||||
| Rat ID Number | Construct Weight (g) | Stimulation Amplitude (mA) | Conduction Velocity (m/s) | V Peak-to-Peak (mV) | Stimulation Amplitude (mA) | Conduction Velocity (m/s) | V Peak-to-Peak (µV) |
| 4607 | 0.087 | 4.17 | 11.3 | 10.3 | 18 | 11.1 | 121 |
| 4608 | 0.15 | 1.65 | 11.1 | 17.1 | 7.7 | 6.5 | 136 |
| 4611 | 0.113 | 8.3 | 9.6 | 11.2 | 10 | 10 | 121 |
| 4613 | 0.116 | 3.18 | 10 | 9.6 | 1.44 | 8.3 | 134 |
| 4614 | 0.189 | 3 | 10.8 | 9.6 | 7.39 | 9 | 151 |
| 4616 | 0.122 | 5.2 | 9.4 | 14.9 | 1.8 | 9.1 | 100 |
| 4620 | 0.118 | 2.91 | 7.6 | 7.4 | 8.7 | 10 | 219 |
| 9 Month Data | CMAP Data (Stimulate CP nerve and record from muscle graft) | CSNAP Data (Stimulate skin graft and record from CP nerve) | |||||
| Rat ID Number | Construct Weight (g) | Stimulation Amplitude (mA) | Conduction Velocity (m/s) | V Peak-to-Peak (mV) | Stimulation Amplitude (mA) | Conduction Velocity (m/s) | V Peak-to-Peak (µV) |
| 4687 | 0.238 | 1.35 | 9.6 | 18.2 | 0.99 | 11 | 181 |
| 4688 | 0.131 | 1.08 | 10 | 8.8 | 1.11 | 8 | 132 |
| 4689 | 0.26 | 1.26 | 9.6 | 21.8 | 1.9 | 8.6 | 237 |
| 4690 | 0.192 | 4.2 | 8.3 | 12.8 | n/a | n/a | n/a |
| 4691 | 0.213 | 1.38 | 10 | 18.6 | 6.6 | 8 | 153 |
| 4693 | 0.178 | 1.11 | 9.6 | 15.1 | 8.7 | 8.3 | 306 |
Table 1: Electrophysiologic testing of C-RPNIs at 3- and 9-months post-construction. To obtain CMAPs, a recording electrode was placed on the muscle with a stimulating electrode on the proximal common peroneal nerve. A series of stimulations increasing in amplitude was applied to the nerve until maximal CMAP values were obtained and results recorded. A similar methodology was applied to the dermal component but with the recording electrode placed on the nerve and stimulating electrode on the dermis. For the sensory evaluation of rat 4690 at 9 months, the dermal graft was found to be too scarred to allow for testing.
Video 1: Muscle contraction within a C-RPNI. A pair of forceps can be seen to the left of the video gently squeezing the proximal common peroneal nerve. This results in contraction of the muscle component of a 3-month-old C-RPNI that is visible to the viewer. Please click here to view this video (Right click to download).