The following results have been published by Pilz et al.6. With this precise surgical procedure, the cardioprotective effect of remote ischemic perconditioning (RIPerc) can be investigated. This is a potential new treatment for patients suffering from acute MI or MIR and subsequent ventricular remodeling, which in many cases leads to consecutive HF. Mimicking the pathophysiological changes of MI/MIR is an obligatory step in the evaluation of treatments as in vitro or ex vivo studies do not provide the physiological environment. In this protocol, the animals were subjected to 30 min of LAD occlusion followed by reperfusion (i.e., MIR).
To prove the reproducibility of the procedure, histological cuts and stains were performed (Figure 4A). It was clear that the fibrotic scar in MIR+RIPerc treated animals was comparable with the scar formation of the Sham animals while the comparison of fibrosis between Sham and MIR groups was significant (Figure 4B). Additionally, MIR+RIPerc treated animals showed significantly reduced fibrosis compared to MIR-treated animals. However, the representative histological images clarify the potency of this surgical procedure as the infarction is explicitly sustained in the MIR group (Figure 4A). Using in vivo echography, ejection fraction, LV end-diastolic and end-systolic diameters (LVEDD and LVESD) were measured and showed significantly reduced cardiac function due to MIR treatment while hemodynamic parameters were preserved by RIPerc (Figure 4C−F). Ex vivo hemodynamic data exhibited the effectiveness of the procedure as the MIR group showed significant decreases in LVSP, cardiac output (CO), stroke volume (SV) as well as external heart work (EHW) (Figure 5A−G).
A literature search about this surgical procedure reported no negative or unsatisfying comments and results when it was adequately performed. Nevertheless, pitfalls mentioned in the introduction and the discussion need to be prevented and training is mandatory to acquire a stable level of performance and to obtain comparable results.
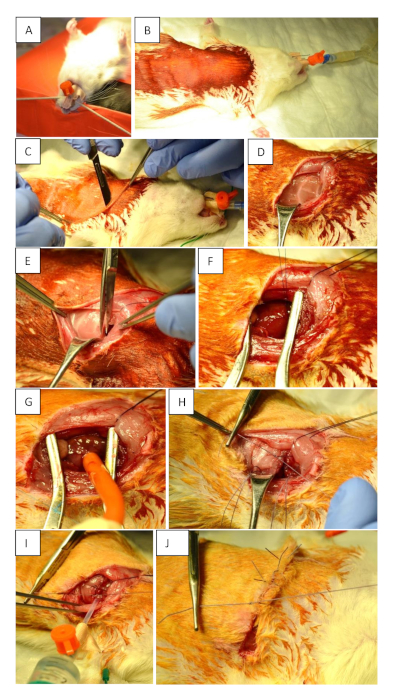
Figure 1: Preoperative preparation and surgical procedure. (A) Intubation of the animal using a 14 G tube. (B) Supine positioning and disinfection of the surgical field. (C) Skin incision (2 mm parasternal on the left thorax at the level of the 3rd intercostal space). The incision must reach the anterior axillary line at the level of the 5th intercostal space. (D) Displace the muscles to make the ribs visible. (E) Opening of the thorax. (F) Permanent occlusion of LAD using 6−7 knots. (G) Transient occlusion of LAD using a tourniquet. (H) Closure of the chest after myocardial ischemia and reperfusion by placing three single-knot sutures around the ribs. (I) Proper closing of the thorax. Use a 10 mL syringe to remove any residual air from the thorax before fixing the last knot tightly. This is integral to prevent a pneumothorax. (J) Skin suture. Please click here to view a larger version of this figure.
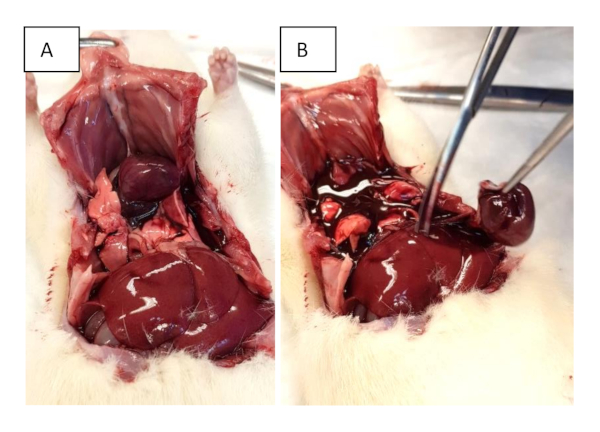
Figure 2: Organ harvesting. (A) Open the chest with sub-xiphoidal cuts and extend them to both mid-axillary lines. Further cuts through the ribs are performed to facilitate lifting of the sternum. (B) Excision of the heart. Please click here to view a larger version of this figure.
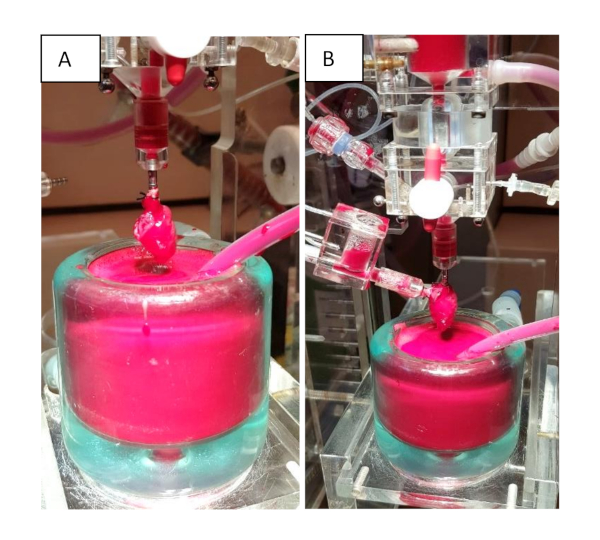
Figure 3: Isolated heart apparatus. (A) Langendorff mode. The heart is mounted to the WH apparatus via cannulation of the aorta. (B) Working heart mode. The system can be switched to the WH model to evaluate cardiac function by cannulating the left atrium. Please click here to view a larger version of this figure.
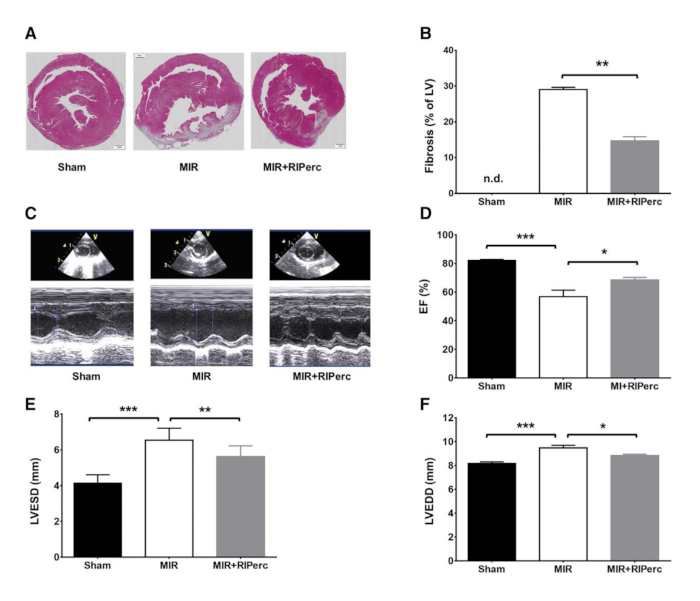
Figure 4: Effect of remote ischemic conditioning on scar formation, left ventricular function and remodeling. (A) Histological LV slices harvested on day 14 post-myocardial reperfusion. (B) Quantified results of fibrosis in bar graphs. (C) Representative M-mode echocardiograms. (D) Ejection fraction (EF) quantified in bar graphs. (E) LV end-systolic diameter (LVESD) quantified in bar graphs. (F) LV end-diastolic diameter (LVEDD) quantified in bar graphs. MIR, myocardial ischemia-reperfusion; RIPerc, remote ischemic perconditioning. Data are expressed as mean ± SEM. *p < 0.05; **p < 0.01; ***p < 0.001. Reprinted from Pilz et al.6 with permission from Elsevier. Please click here to view a larger version of this figure.
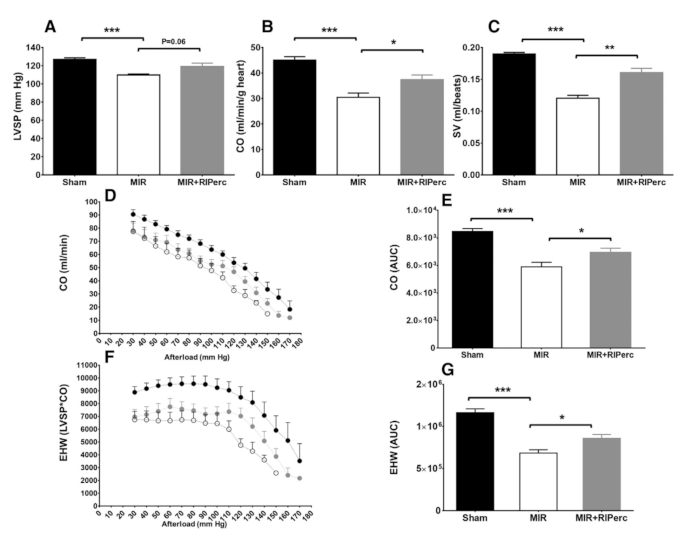
Figure 5: Effect of RIPerc on LV hemodynamic function. (A) LV systolic pressure (LVSP), (B) cardiac output (CO), and (C) stroke volume (SV) results were obtained from the isolated working heart on day 14 post-myocardial reperfusion. (D) CO is depicted as a function of afterload; (F) external heart-work as function of afterload, quantified results in bar graph (E and G). Data is expressed as mean ± SEM and n = 4–7 per group. *p < 0.05; **p < 0.01; ***p < 0.001. MIR, myocardial ischemia/reperfusion; RIPerc, remote ischemic preconditioning; EHW, external heart work; SV, stroke volume; AUC, area under the curve. Reprinted from Pilz et al.6 with permission from Elsevier. Please click here to view a larger version of this figure.
