Successful ultrasound-microbubble treatments can be detected by the extravasation of fluorescent dextran from the intravascular to the extravascular space (Figure 8), indicating an increase in BBB permeability. Depending on the pressure field of the ring transducer, pial vessels and/or capillaries will be affected.
To evaluate the vascular changes induced by ultrasound-microbubble treatments, the diameter of the vessel of interest can be measured before, during, and after ultrasound-microbubble treatment (Figure 9). This can be done manually in a commercially available software (e.g., Olympus Fluoview software). During image acquisition, bolus dextran injections and line scans can also be used to assess blood flow30,41. To evaluate kinetics of dextran leakage as a representative model for drug delivery, the signal intensity between the intra- and extravascular spaces can be evaluated using tools such as MATLAB26,27,29,41 (Figure 10).
Further image processing can be achieved using ImageJ/FIJI. ImageJ/FIJI is an open-source software that is compatible with MATLAB and is well-suited to conduct common analyses in biological image analysis, such as measuring vascular changes, or the lengths of or distance between fluorescent objects (e.g., β-amyloid plaques to blood vessels). Image processing pipelines created in ImageJ/FIJI can be automated by writing custom macros.
More complex analyses, such as 3D segmentation of blood vessels and cell tracking, can be achieved using more advanced, semi-automated software (Figure 11). Following segmentation, more specific analyses can be conducted, such as classifying blood vessels as arterioles, venules, or capillaries, based on diameter, branching, tortuosity patterns, and flow direction42,43. Machine learning algorithms have also been developed to automate blood vessel segmentation22,44.
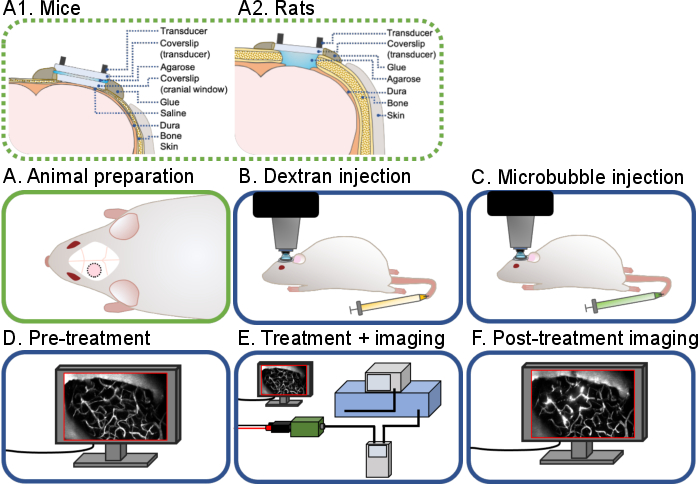
Figure 1: General workflow of intravital multiphoton ultrasound-microbubble brain experiments. A general workflow of the intravital multiphoton ultrasound-microbubble brain experiments described in this protocol is shown. There are 6 steps: (A) Animal preparation for (A1) mice and (A2) rats, (B) Dextran injection, (C) Microbubble injection, (D) Pre-treatment imaging, (E) Treatment and imaging, (F) Post-treatment imaging and data analysis. Please click here to view a larger version of this figure.
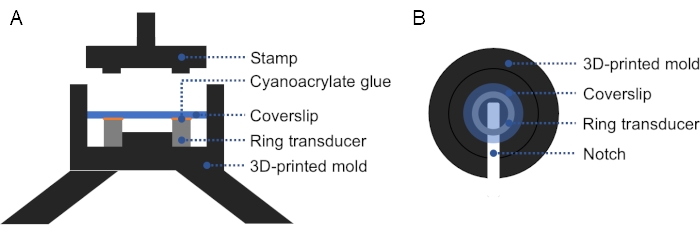
Figure 2: Cross-section and top view of 3D-printed mold. (A) Cross-section of the mold. A thin layer of cyanoacrylate glue is applied on the top surface of the ring transducer, and a coverslip is placed on top. A stamp may be used to apply firm, even pressure on the coverslip and ring transducer. (B) Top view of the mold. A notch can be added in the mold to facilitate removal of the prepared transducer. Please click here to view a larger version of this figure.
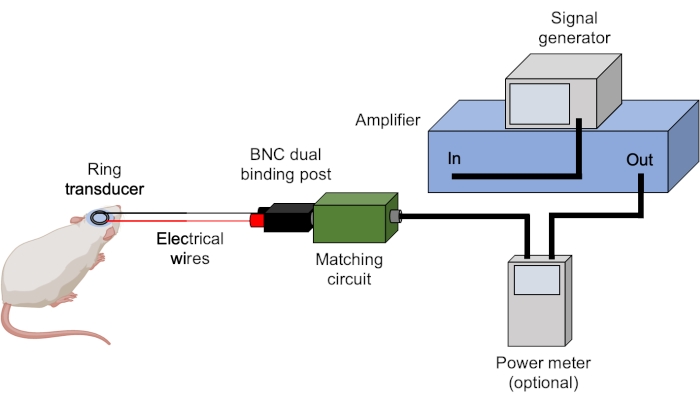
Figure 3: Ultrasound set-up. Typical hardware for ultrasound experiments are shown. Ultrasound parameters are set and triggered by the signal generator and amplified by the amplifier. A power meter can be used to record forward and reflected powers prior to sending the signal to the matching box, which is matched to the transducer. All connections are achieved using BNC cables unless stated otherwise. Please click here to view a larger version of this figure.
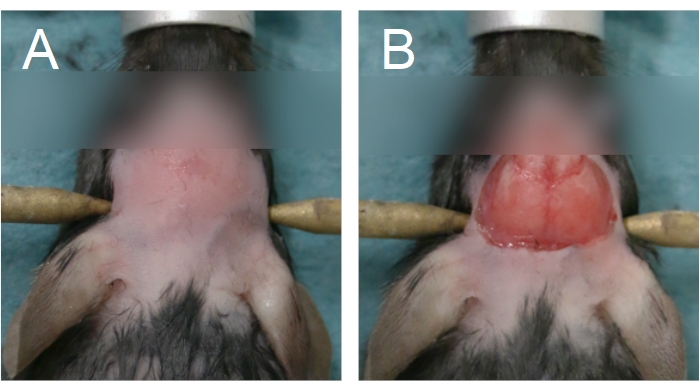
Figure 4: Area of fur removal and scalp removal. (A) Fur removal should start from between the eyes and extend until the anterior half of the neck. (B) Scalp removal should be sufficient to expose the parietal bones. Bleeding must be stopped before proceeding. Please click here to view a larger version of this figure.
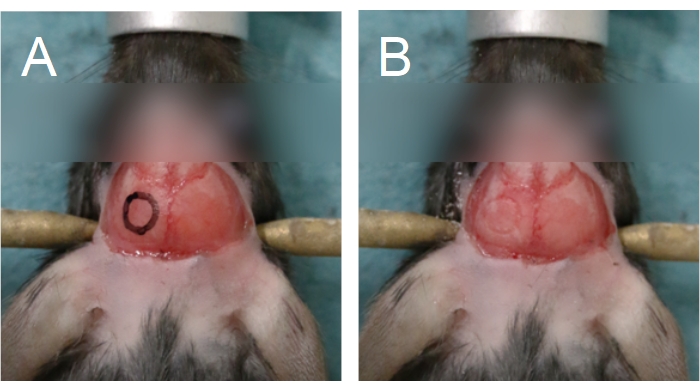
Figure 5: Outline of the cranial window. The cranial window is situated on a parietal bone. (A) An outline of the cranial window can be drawn onto the skull to aid in the drilling process. (B) The outline of the cranial window can be seen following drilling through the compact bone. Please click here to view a larger version of this figure.
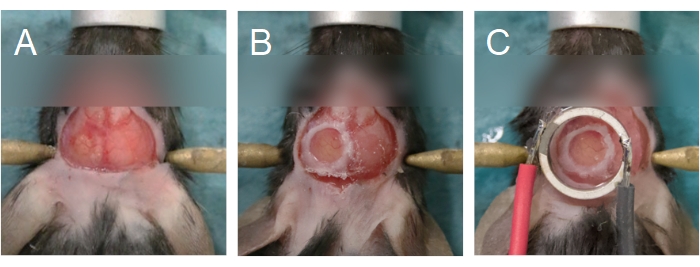
Figure 6: Cranial window and transducer alignment. (A) The cranial window is created on a parietal bone. The bone island has been removed, exposing the brain underneath. (B) The cranial window is complete when a glass coverslip is sealed onto the skull using cyanoacrylate glue. (C) The transducer is centered to the cranial window and adhered using cyanoacrylate glue. Please click here to view a larger version of this figure.
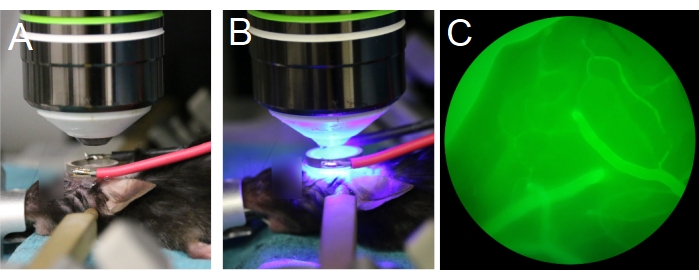
Figure 7: Positioning of objective lens and transducer. (A,B) The objective lens is centered to the ring transducer. (C) Blood vessels filled with fluorescent dextran are visible through the eyepieces, under epifluorescence. Please click here to view a larger version of this figure.
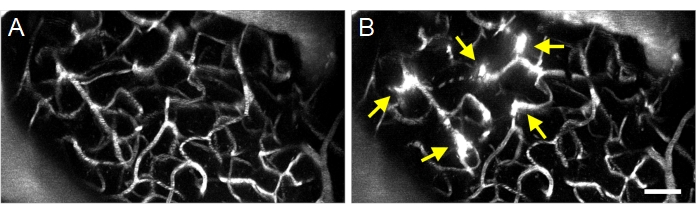
Figure 8: Maximum projection multiphoton images of ultrasound-microbubble induced increases in BBB permeability. Maximum projection images of vasculature (A) before and (B) after ultrasound-microbubble treatments. Successful ultrasound-microbubble treatments can be confirmed by observing increases in BBB permeability following treatment, visualized as fluorescent dextran extravasation (arrows). Scale bar: 50 µm. Please click here to view a larger version of this figure.
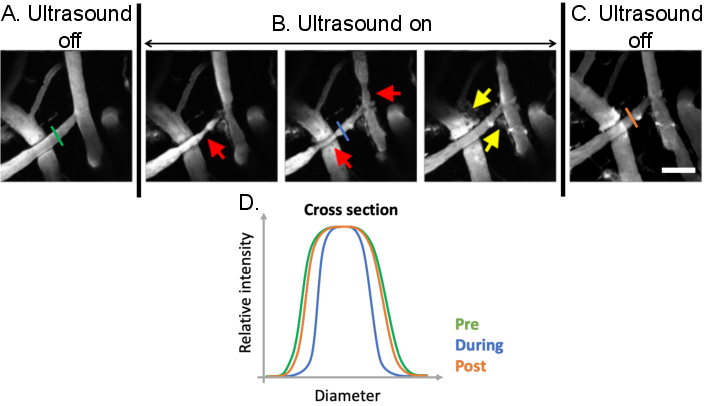
Figure 9: Analysis of vasomodulation induced by ultrasound-microbubble treatments. Maximum projection images of cerebral blood vessels before, during, and after ultrasound-microbubble treatments. Microbubbles are present in all images. Compared to (A) pre-treatment conditions, clear vasomodulation can be observed (B) during ultrasound-microbubble treatments (red arrows). Ultrasound-microbubble mediated increases in BBB permeability are also evident following treatment from the leakage of fluorescent dextran from the intravascular to the extravascular space (yellow arrows). (C) When ultrasound is turned off, vascular diameters return to pre-treatment, baseline sizes. (D) Vascular changes can be analyzed by plotting the diameter of the vessel of interest before, during, and after ultrasound-microbubble treatment. Scale bar: 100 µm. (Unpublished work). Please click here to view a larger version of this figure.
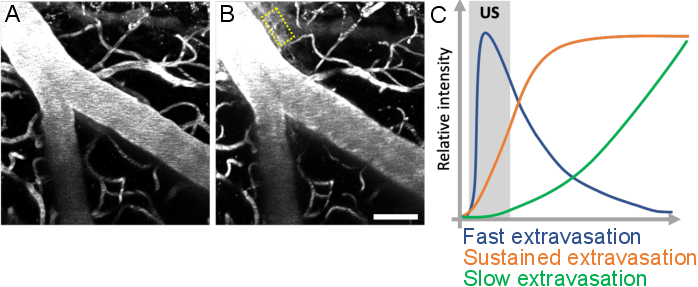
Figure 10: Analysis of leakage kinetics following ultrasound-microbubble treatments. Increase in BBB permeability is visualized as leakage of fluorescent dextran from the intravascular to the extravascular space. Changes in BBB permeability are evident when comparing image stacks acquired (A) before and (B) after ultrasound-microbubble treatments. (C) Leakage kinetics can be analyzed by tracking the intensity, volume, and speed of dextran in extravascular compartments (yellow rectangle). Scale bar: 50 µm. (Unpublished work.) Please click here to view a larger version of this figure.
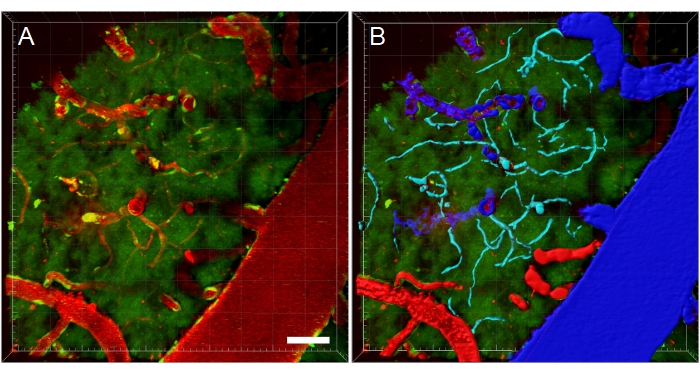
Figure 11: Blood vessel segmentation of multiphoton microscopy XYZ stack. (A) Depth (XYZ) stack of blood vessels in a transgenic EGFP rat. Blood vessels are visualized via intravenous injection of fluorescent Texas Red 70 kDa dextran (red). The green channel shows fluorescent cells and tissue autofluorescence. (B) 3D reconstructions of blood vessels are created, and then color-coded according to blood vessel type to facilitate type-specific analyses. Vein/venules are blue, arteries/arterioles are red, and capillaries are cyan. Scale bar: 50 µm. Reconstructions created using Bitplane Imaris. Please click here to view a larger version of this figure.
