The rationale for the use of serum-derived eye drops (which is the blood-based product most frequently used for the treatment of eye surface diseases) lies in their content of GFs, which are almost completely derived from circulating platelets. PRP contains a significantly higher number of platelets (and, consequently, of platelet-derived GFs) compared to peripheral blood serum, ranging between 0.15 x 109-0.45 x 109 PLTs/mL. According to Italian laws, the platelet count in PRP units should be at least 0.9 x 109-1 x 109 PLTs/mL. Therefore, to obtain a product that simulates the efficacy of serum eye drops, PRP should be diluted to the physiological platelet content before lysate preparation.
Nevertheless, since tissue repair is mainly driven by platelet-derived GFs, the PLT scount alone might be misleading for an effective therapy of eye surface diseases. In DED, which is the eye disease most commonly treated with blood-derived eye drops, tear film production and homeostasis are impaired. Platelet-based products for the treatment of DED, therefore, should also mimic the physiological content of tears.
To identify the most suitable PRP-L for treating eye surface diseases, described in step 1.3.2. of the present protocol, we preliminarily assessed different PRP dilutions, according to their PLTs content (between 0.7 x 109/mL and 0.3 x 109/mL), and some representative GFs from those that are known to be involved in eye tissue repair12,20,21.
Platelet count was performed with a hemocytometer, while GFs were assessed by means of a multiplex protein quantification assay. The assay was performed as previously described25 according to the manufacturer's instructions. GFs shown in this manuscript were selected for quantification after a preliminary screening of 36 GFs and GFRs performed on PRP lysate with a semi-quantitative protein array. Luminex quantification was performed on 3 out of the 36 screened GFs: EGF and PDGF (which turned out to be the most abundant ones in our PRP lysates) and TGFβ-1,2,3 isoforms (for which the content is important for the eye surface treatment21). EGF and PDGF content were measured as they may influence the efficacy of PRP-L22, while TGFβ isoforms were selected for their known role in immune signaling regualtion21.
Since protein arrays are part of another in vitro study on the characterization of different PRP26, those data are not presented in this manuscript.
We quantitatively assessed EGF, PDGF, and TGFβ in PRP lysates from two different donors (D1 and D2), previously diluted between 0.7 x 109-0.3 x 109 PLTs/mL in 0.9% NaCl. Figure 2 shows the results of the 0.3 x 109 PLTs/mL dilution, which turned out to be most similar to tear composition.
The 0.3 x 109 PLTs/mL dilution was selected based on literature data on tear composition. The EGF values were found to be quite low compared to the mean tear value but still in the range of normality27. Even PDGF, despite being highly variable between the two donors considered, was always comparable to the concentration found in normal tears20. Finally, TGFβ-1 was found to be the most abundant isoform in PRP-L, similar to tears21.
Once the most suitable PLT dilution to prepare apheresis PRP-L had been identified, the Transfusion Medicine Unit started distributing these products to patients affected by eye surface disorders in 2015. The ophthalmologists routinely collected the OSDI questionnaires to monitor DED symptoms; the OSDI test assesses quality of life measures, such as the perception of ocular irritation and how it affects the functioning related to vision. The questionnaire, created by the Outcomes Research Group at Allergan Inc. in 1995 and now accepted as a valid instrument to monitor DED, is submitted to patients and analyzed as previously described28,29.
Here, we show the aggregate results of OSDI tests of DED patients treated between January 2020 and January 2021 (n = 27). After a 6 month therapy with PRP-L, the OSDI scores decreased from 56 ± 21 to 45 ± 21, indicating an improvement in patients' quality of life (Figure 3).
Despite these data still being in the severe range and not relating to clinical outcomes of efficacy, they suggest that DED patients consider PRP-L a useful product that ameliorates ocular discomfort; this aspect should be further investigated in prospective clinical trials aimed at assessing its efficacy in treating ocular surface diseases.
In Table 1, we report a comparison of the present method of production with another method for preparing allogenic PRP-L for eye drops30 and for other purposes22. To our knowledge, Zhang's30 protocol and the current protocol are the only published methods to produce PRP-L for the eye surface. In both, PRP-L is obtained from apheresis; differences between the two protocols, mainly relating to the number of freeze and thaw cycles and centrifugation steps, should be compared in order to improve PRP-L production. Nevertheless, these methodological differences have not been proved to be detrimental to the regenerative capacity of PRP-L tested on other tissues22.
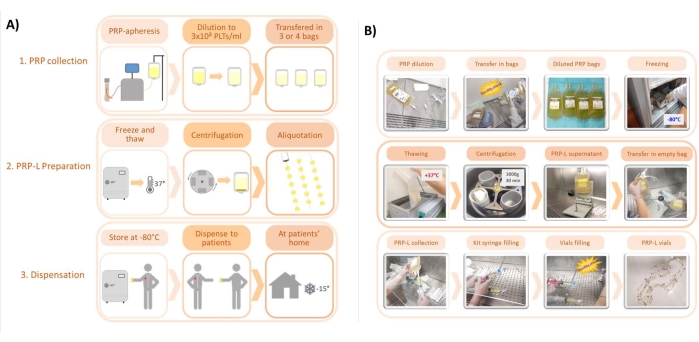
Figure 1: Main steps of the protocol for the preparation of PRP-L. (A) Scheme of the protocol, from PRP collection to PRP-L preparation and dispensation. (B) Representative pictures of the main steps of the protocols. Please click here to view a larger version of this figure.
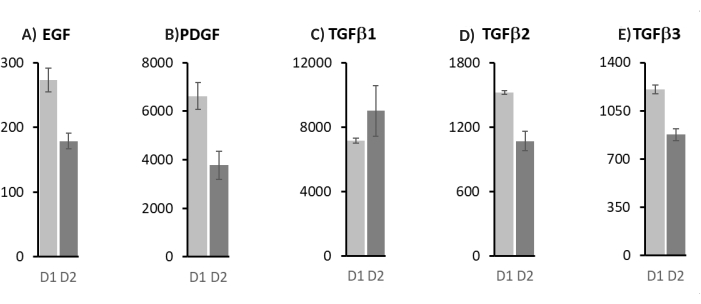
Figure 2: Luminex quantification of platelet-derived growth factors for the 0.3 x 109/mL dilution of PRP-L. (A) Epidermal growth factor (EGF); (B) platelet-derived growth factor (PDGF); (C) transforming growth factor-beta isoform 1 (TGFβ1); (D) transforming growth factor-beta isoform 2 (TGFβ2); (E) transforming growth factor-beta isoform 3 (TGFβ3). Values are expressed as pg/mL, mean ± standard deviation of three independent measurements. D1 and D2 are two different platelet donors. Please click here to view a larger version of this figure.
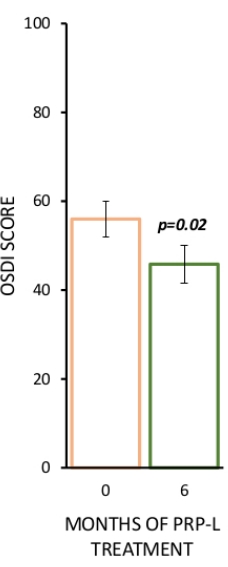
Figure 3: Aggregate OSDI scores of DED patients treated with PRP-L between January 2020 and January 2021 at the Ophthalmology Unit of the AUSL-IRCCS di Reggio Emilia. N = 27 patients. OSDI score aggregate results are represented as mean ± standard error, p-value was calculated with a paired t-test with data analysis software. Please click here to view a larger version of this figure.
| This article | PRP-L for the eye (in vitro study)29 | PRP-L for other purposes21 | |
| Source | PLTs apheresis | PLTs apheresis | Apheresis and whole blood |
| Freeze and thaw cycles | 1 (at -80 °C) | 2 (at -80 °C) | 1-3 (at -20 °C and -80 °C) |
| Storage temperature | at -80 °C | at -80 °C | at -20 °C and -80 °C |
| Centrifugation speed before storage | 3000 x g/30 min | 3500 x g/30 min | 400-3000 x g/6 min -30 min |
| Filtration before storage | No | Yes | No/Yes |
Table 1: Comparison of protocols to prepare allogenic PRP-L from platelet-based products collected by apheresis.