After following the step-by-step procedure, the delivery of a suprathreshold TMS pulse (120% of the RMT) will elicit an observable MEP in the EMG recording of the target muscle, and a subsequent period of background EMG activity suppression of approximately 150 ms to 300 ms (Figure 2). From that EMG pattern, it's possible to calculate the cSP metrics. The most reported outcomes are the duration (in the range of ms) of the relative and absolute SP. The relative SP is measured from the MEP start to the reappearance of EMG activity. One alternative is using the amplified motor stimulated output (MSO = 120% of RMT, as per the protocol) to establish the onset of relative SP. Since the true onset at a network level cannot be known, select the MEP onset as the initial start point to increase experimental reliability13. On the other hand, the absolute SP can be measured from the end of the MEP to the onset of the reemergence of voluntary EMG activity. For instance, using a recording of the resting EMG activity of the subject as reference for qualitative comparison. Those temporal parameters can be identified manually or using automated software37.
A fundamental methodological question for accurate cSP calculation is the definition of the reemergence of EMG background activity. Two approaches can be explored here: The first is using individual trial calculation. In this case, the calculation is based on trial-by-trial measure, using each recording to calculate the cSP duration. Then, a mean (or median) of the individual trials can be calculated and reported. The second approach is using rectified multiple trials. For this approach, all trials will be rectified, and then have to be averaged and overlapped with each other. Then, using the rectified and averaged traces, calculate the cSP duration using average temporal marks. The main advantage of this method is its precision and easier identification of the reappearance of voluntary EMG activity relative to the tonic baseline EMG level36. Using rectified average is advantageous because it is more comparable and reduces the between-subject variability.
It is important to mention that the cSP duration can be prolonged as a sigmoid function of stimulus intensity38, but it is barely affected by the degree of intentional contraction of the target muscle39. Moreover, MEP amplitudes increase with increases in stimulus intensities. Kojima et al. demonstrated that these increases in MEP amplitude (secondary to increases in intensity) is also accompanied by increases in cSP duration40. This behavior is expected since the MEP and cSP duration are thought to be influenced by common factors38. These common factors seem to be present throughout the cortical spinal tract and not in the motor unit; since the increases in stimulus intensity increases both, but increases in muscles contraction do not affect the cSP duration.
With this discussion, it is possible to conclude that stimulus intensity and muscle contraction must be carefully considered during the analysis and interpretation of findings. The cSP is characterized by a linear increase due to the SI, but then a plateau is reached at high intensities; this pattern is highly variable across subjects39, since they could have unique slopes and different plateau intensities. One alternative analysis could include evaluating the cSP during progressively increased intensities to perform an input-output (I/O) curve, and then the cSP can be obtained using the intensity at which the I/O curve reaches the plateau41,42. Finally, since cSP is affected by any activity or exposure that can produce cortical excitability and inhibition changes, it is recommended to assess and record general confounders in the analysis. For instance, using a reporting checklist for TMS experiments43.
cSP interpretation
The TMS test in the current study was used to show the implementation of a feasible and versatile biomarker of M1 inhibition. In general, the longer the duration of the SP, a higher corticospinal M1 inhibition is observed44. However, several factors need to be considered for its interpretation. First, the cSP is defined by both spinal and cortico-subcortical processes45. The spinal components account for approximately the first 50 ms46. The remaining duration is highly influenced by cortical mechanisms such as M1 interneurons inhibition and other inhibitory afferences within M1 (from subcortical regions and other cortices), mediated mainly by GABAergic B neurons after an important cortical activation eliciting MEPs6. It has been suggested that the role of this inhibition is to prevent unwanted movements and sustain motor control47. Second, behavioral and cognitive factors can impact the CSP duration, as well as motor and non-motor neuropsychiatric disorders45,48. Due to this dual nature of cSP, its values need to be interpreted within the experiment context (target population and the use of concomitant motor control tasks).
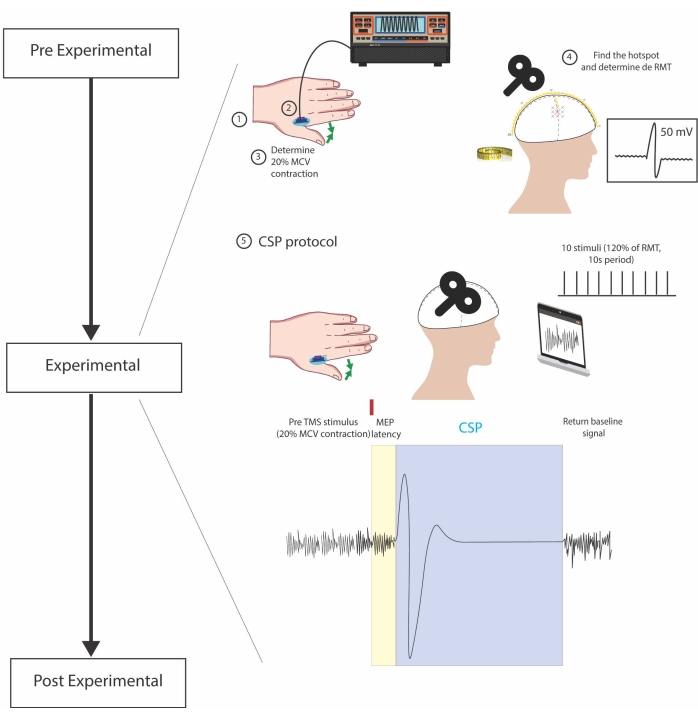
Figure 1: Experimental steps. 1. Electrode placement on the belly of the FDI muscle 2. Positioning of the dynamometer between fingers. 3. Voluntary contraction of the target muscle to test the standardization of 20% MVC 4. Head measurements and TMS pulses for identification of the hotspot and the RMT (lowest stimuli that elicits an MEP of at least 50 mV in five out of ten trials) 5. CSP protocol, consistent of 10 pulses with 120% RMT spaced out by 10s, during sustained muscle contraction. In the bottom center figure, the small red rectangle represents a single TMS pulse and divides pre-TMS stimulus (sustained muscle contraction and background EMG activity) and the cSP recording. CSP is considered from the start of the MEP until the reemergence of EMG baseline activity, represented inside the blue rectangle. In the yellow rectangle, the MEP latency is shown. Please click here to view a larger version of this figure.
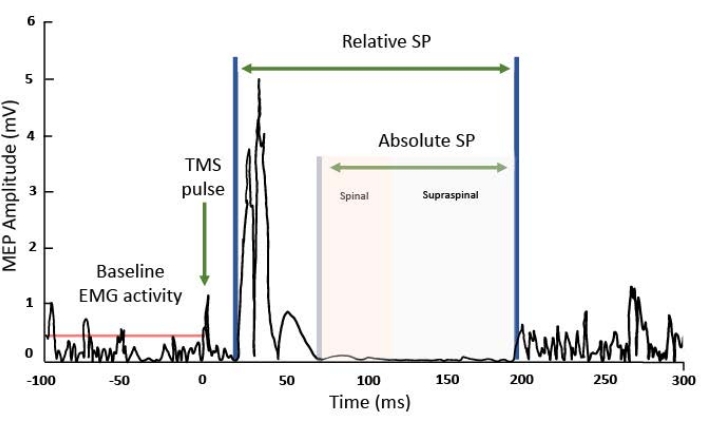
Figure 2: MEP in the EMG recording of the target muscle. On the X-axis, milliseconds (ms), and the Y axis, millivolts (mV) of the EMG signal. From left to right: the red line indicates the background electrical muscle activity before the MEP, subsequently, after the electric effect of the TMS pulse is observed it is followed by the motor-evoked potential. After the MEP, there is a suppression of the EMG signal known as the SP. It can be relative, counting the interval from the beginning of the MEP wave to the return of EMG background activity or absolute SP, counting the interval from the end of the MEP to the return of the background wave. Please click here to view a larger version of this figure.
