To elucidate the practical use of this method, the right mandibular first molar of two healthy C57BL/6 mice (3 months old, both female) were extracted and followed for 1 week and 4 weeks, respectively. The undamaged left mandibles were used as healthy controls. Figure 1A shows the specific features of the surgical appliance, including 26-23 G needles and a toothed ophthalmic tweezer. The 26 G needle is pinpoint-removed and bent. The 25 G needle is bent at approximately 25° at the pinpoint. The 23 G needles are the linchpin for the surgery and are bent at approximately 25° and 35°, respectively, at the pinpoint (Figure 1B1,B2). The tweezers have a 1 mm long tooth that fits the shape of the murine molars (Figure 1B3). Figure 1C shows the state of the mouse before surgery. The key points are the location of the four pins around the head and fixing the tongue under the rubber band on the left.
Figure 3A shows the position and morphology of the right mandibular first molar. Figure 3B indicates the tooth socket immediately filled with clot post-extraction. At 1 week and 2 weeks, the mice were euthanized, and the mandibles were demineralized, embedded in paraffin17, and sectioned into slices. Figure 4A displays the healing process of the socket at 1 week. Some sponge-like trabecular bones were formed, but the clot remained. In the healing process at 2 weeks (Figure 4B), the socket was fully filled with sponge bones, meaning the regeneration was roughly completed. The immunofluorescence (IF) staining also corroborated the results of the histopathology staining. In Figure 5, the Sp7 was widely expressed in the bone marrow cells, especially in the margin, which is the bone-forming front. Under the homeostasis state, the trabecular bones were consistent and confluent, with bone marrow cell blocks sprinkled like islands. However, at 1 week post-surgery, numerous Sp7-expressing cells filled the extraction socket, with newly formed trabecular bone sprinkled around. At 4 weeks post-surgery, the condition reversed and turned to largely merged trabecular bone again, and the activity of Sp7-expressing cells declined to a level approaching the homeostasis state.
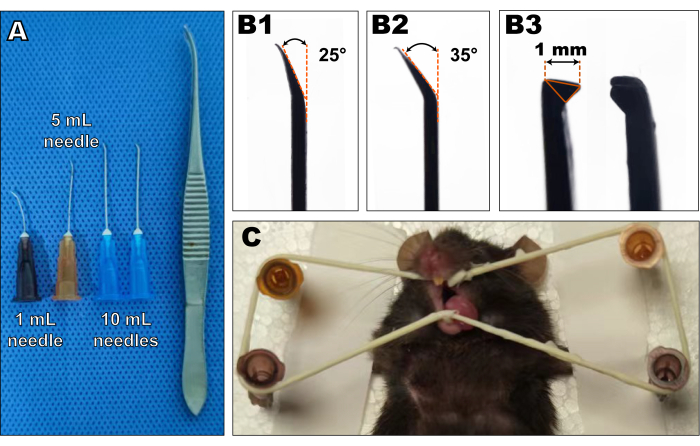
Figure 1: The object images of surgical appliances and surgery-prepared mice. (A) The surgical appliances mainly consisted of 26, 25, and 23 G needles and a toothed tweezer. (B) Needles were bent at the pinpoint at 20°-40° (B1,2). The tweezers' tooth must be approximately 1 mm in size (B3). Please click here to view a larger version of this figure.
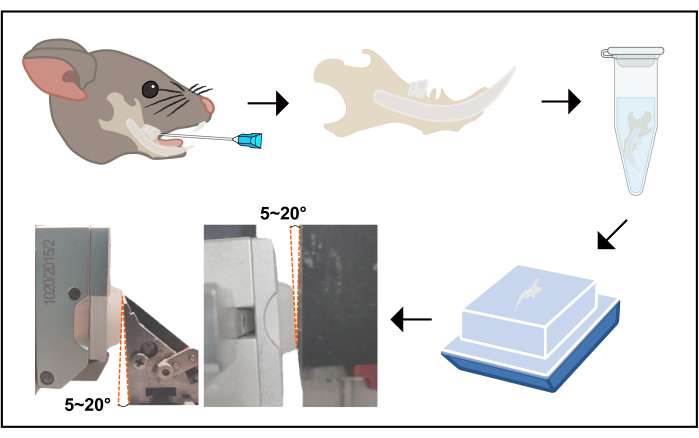
Figure 2: The flowchart of the procedure from tooth extraction to sectioning. This image displays a schematic flow from tooth extraction to sectioning. The right mandibular first molar was extracted according to the protocol, then the mouse was euthanized, and the mandible was harvested. Upon harvesting, the mandible was soaked in 4% POM for 24 h, then re-soaked in 10% EDTA; the fluid was renewed every day for 14 days. Next, the samples were dehydrated and embedded in paraffin following a universal protocol. The buccal or lingual side must be face down, as sagittal plane slices are supposed to be sectioned. Finally, when fixing the sample on the specimen clamp, the condyle and crown sides must be 5°-20° protruded. Abbreviations: POM = paraformaldehyde; EDTA = ethylenediamine tetra-acetic acid. Please click here to view a larger version of this figure.
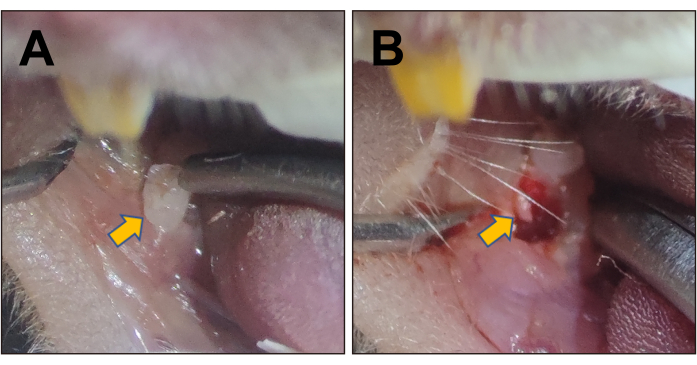
Figure 3: Stereoscopic images of the mouse mandibular first molar and the extraction socket. (A) Stereoscopic image of the right mandibular first molar, indicated by the yellow arrow. (B) The extraction socket of the first right mandibular molar post-surgery, indicated by the yellow arrow. Please click here to view a larger version of this figure.
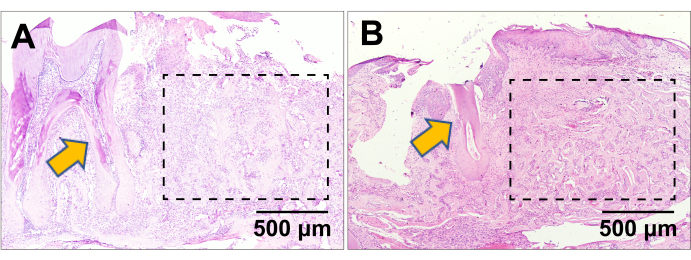
Figure 4: H&E staining. H&E staining of the extraction socket at (A) 1 week and (B) 4 weeks post-surgery. The yellow arrows indicate the mandibular second molar in the proximity of the first molar extraction socket healing. The dashed rectangle line indicate the healing first molar extraction socket area. Scale bars: 500 µm. Please click here to view a larger version of this figure.
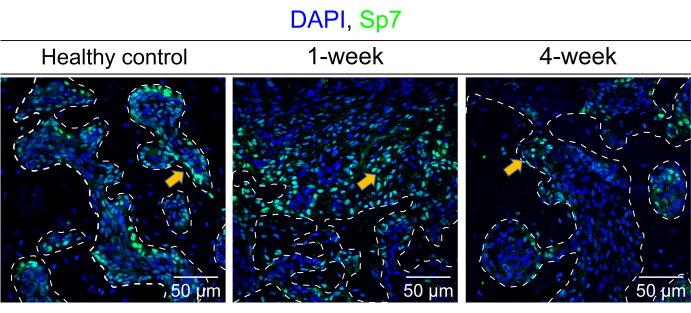
Figure 5: Detection of Sp7 via IF staining. This image shows the distribution of Sp7 expression in the mouse mandible bone marrow cells and the surrounding trabecular bone under a homeostasis state (healthy control), 1 week and 4 weeks post-surgery, respectively. The white dashed line contoured the estimated scale of the trabecular bone. The yellow arrows indicated the typical Sp7-expressing cells. Scale bars: 50 µm. Please click here to view a larger version of this figure.
