The LBNP procedure causes a reduction in air pressure around the lower torso and legs. As this vacuum is progressively increased, blood volume shifts from the head and upper torso to the lower body to create a state of central hypovolemia. The progressive reduction in central blood volume (i.e., LBNP) produces significant alterations in the features of the arterial waveform measured with the infrared finger photoplethysmograph (Figure 5). The Compensatory Reserve Index (CRI) is calculated from the recorded arterial pulse wave using a unique machine learning algorithm which analyzes changes in wave form characteristics to calculate an estimated compensatory reserve (Figure 6).1,15,16 Each continuous noninvasive photoplethysmograph waveform (represented as the monitored 'Patient's Arterial Waveform') is the input to calculate an estimate of an individual's compensatory reserve (represented as the 'CRI Estimate') based on comparison to a large 'library' of reference waveforms (represented as the 'Algorithm Waveform Library') generated from progressive levels of central hypovolemia.
In this experiment, a subject was exposed to LBNP until the onset of hemodynamic decompensation which occurs when the body is no longer able to compensate for the hypovolemia. The values for mean arterial pressure, heart rate, SpO2, and CRI plotted against time (i.e., progressive reductions in central blood volume caused by increasing levels of LBNP) are shown in Figure 7. The results of the experiment show that changes in mean arterial pressure, heart rate, and SpO2 occur during the later phases of hemorrhage (i.e., >15 min into the protocol for heart rate and >25 min for mean arterial pressure and SpO2) while CRI decreases early and progressively throughout the multiple steps of LBNP.
Tolerance to reduced central blood volume is defined as the time from the start of the experiment to decompensation. In this example, tolerance was approximately 27.5 min at a level of -70 mmHg LBNP. Based on previous experiments that were designed to equate the magnitude of actual blood loss with LBNP,8 the equivalent blood loss that our subject was able to tolerate was estimated at approximately 1.2 L.
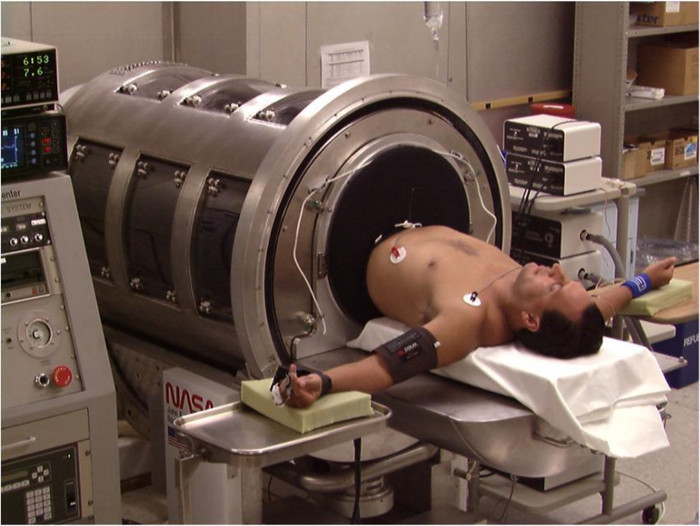
Figure 1: LBNP Chamber. A subject is shown in a supine position on the bed of the LBNP chamber. The neoprene skirt around the subject's waist is used to create an airtight seal within the LBNP chamber. Previously published in Cooke et al.17 Please click here to view a larger version of this figure.
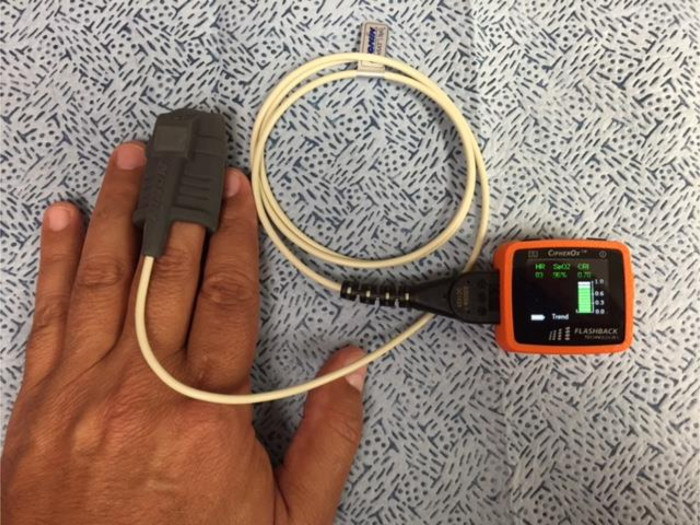
Figure 2: Compensatory Reserve Monitoring Device. The device consists of a noninvasive finger pulse oximeter that transmits pulse oximeter and waveform data via a USB connection to a compensatory reserve monitor. The monitor unit contains an algorithm which calculates a value for compensatory reserve known as the Compensatory Reserve Index (CRI)1,12. Data are recorded at each heart beat and displayed on the monitor and stored on a memory card. Please click here to view a larger version of this figure.
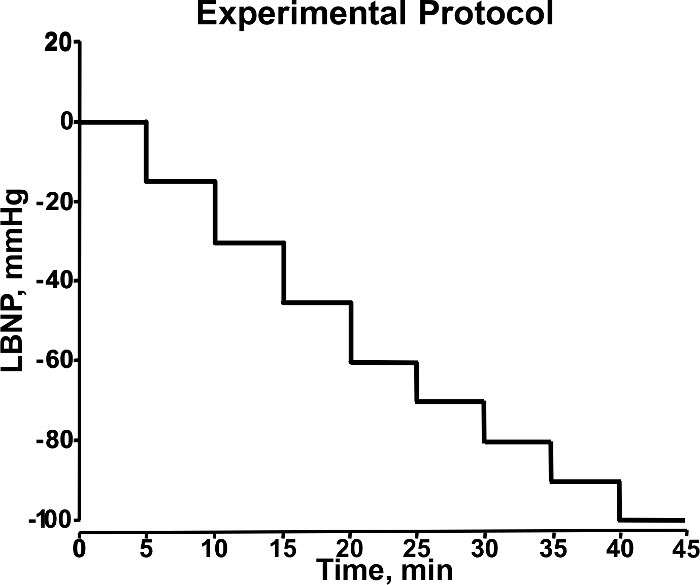
Figure 3. Stepwise Changes in LBNP During Experiment. During the experimental protocol, LBNP (mmHg) is adjusted in a stepwise manner (5 min/level) to induce progressive central hypovolemia. This diagram shows LBNP increasing from 0 to -100 mmHg during 40 min of an experimental protocol. Modified from Convertino et al.18 Please click here to view a larger version of this figure.
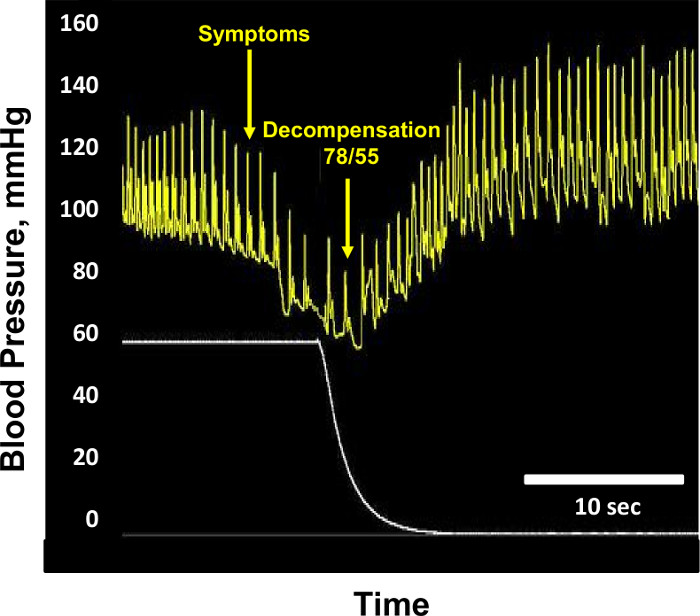
Figure 4: Hemodynamic Decompensation. Sample blood pressure (mm Hg, yellow tracing) and lower body negative pressure (mmHg, white tracing) recordings are shown from a subject at the point of hemodynamic decompensation. At the point of decompensation, blood pressure is 78/55 mmHg, and lower body negative pressure is -60 mmHg. Blood pressure returns to normal after cessation of lower body negative pressure. Modified from Convertino et al.1 Please click here to view a larger version of this figure.
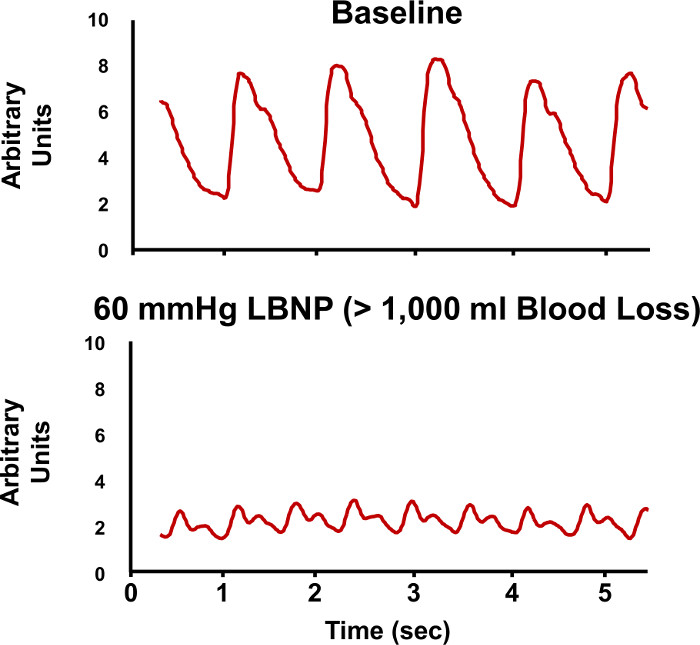
Figure 5. Arterial Waveforms During LBNP. Sample recordings of arterial pressure waveforms are shown during baseline (upper tracing) and during -60 mmHg lower body negative pressure (LBNP, lower tracing). The changes in the characteristic features of the arterial waveforms are evaluated to estimate compensatory reserve. Please click here to view a larger version of this figure.
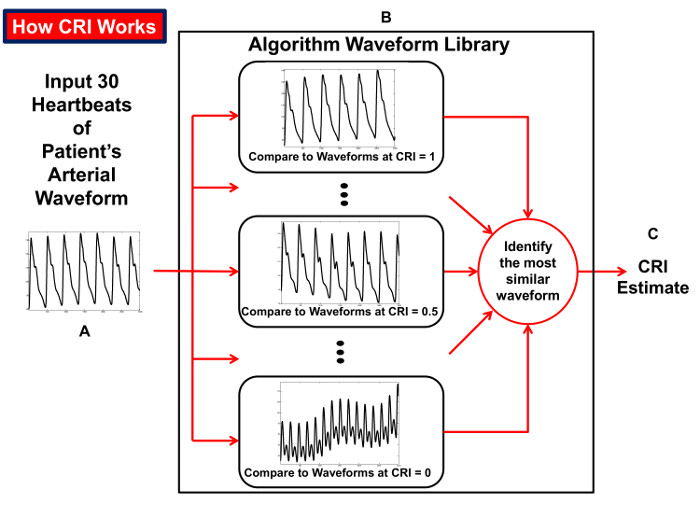
Figure 6: How the CRI is Calculated. Diagram illustrating the process of the compensatory reserve index (CRI) algorithm that compares beat-to-beat arterial blood pressure waveform tracings over an interval of 30 heartbeats (A) to a 'library' of waveforms (B) collected from humans exposed to progressive reductions in central blood volume for generation of an estimated CRI value (C). Reproduced from Convertino et al.15 Please click here to view a larger version of this figure.
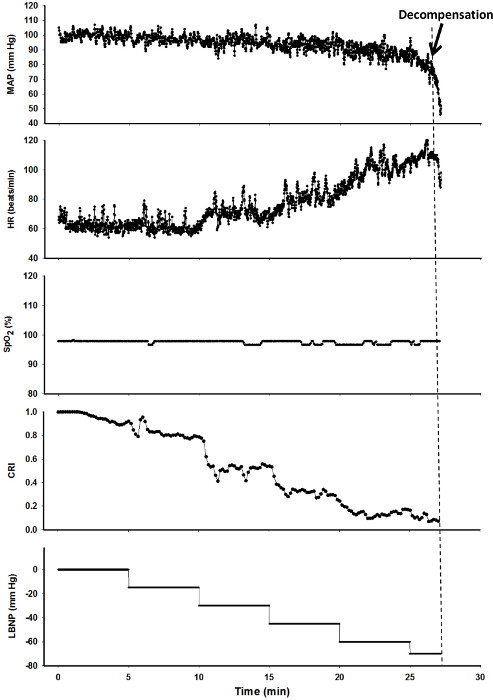
Figure 7. Sample Results of an LBNP Experiment. Values of Mean Arterial Pressure (MAP, mmHg), Heart Rate (HR, beats/min), arterial oxygen saturation (SpO2, %), Compensatory Reserve Index (CRI) and Lower Body Negative Pressure (LBNP, mmHg) are shown for one subject during an LBNP experiment. The dashed line represents the onset of cardiovascular decompensation, Please click here to view a larger version of this figure.
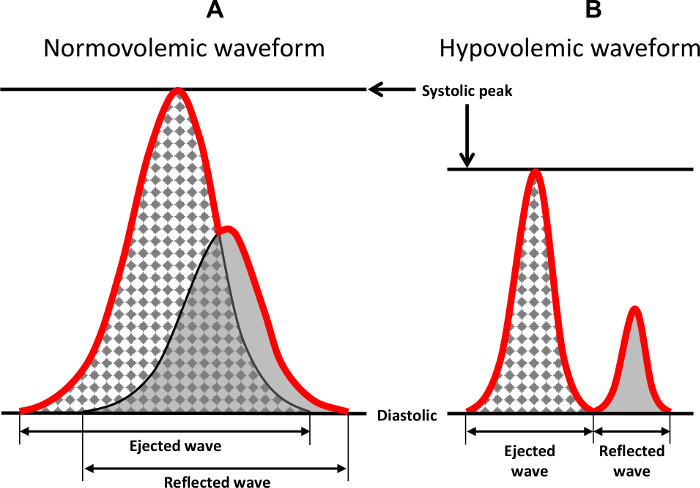
Figure 8: Characteristic Features of the Arterial Waveform. Two wave forms are shown that demonstrate the characteristic features of the arterial ejected and reflected waveforms during normovolemia and hypovolemia. The red line indicates the integrated waveform that is recorded and observed in a tracing. Previously published in Convertino et al.1 Please click here to view a larger version of this figure.