Particles in this size range (1-5 μm) and flow conditions (1-10 L/min) follow the fluid stream lines based on both their theoretical Stokes number and in vivo data; therefore, in the absence of a targeted delivery device, particles released into the lung model are expected to deposit according to the percentage of total airflow diverted to each lobe. The relative amounts of particle delivery to each lobe can then be compared to clinical lobe flow rate data obtained through analyzing patient-specific high-resolution computed tomography (HRCT) scans10. A validated experimental set-up will yield a non-targeted particle deposition profile that has no statistically significant difference from the clinical air flow profile. Validation data is presented for two distinct flow conditions: 1 L/min in a healthy lung (Figure 4A) and 1 L/min in a lung affected by COPD (Figure 4B). Under both these conditions, the experimentally determined deposition profile was not statistically different from the clinical data, demonstrating that the set-up accurately mimics the distribution of air flow to each of the lung lobes. These baseline deposition profiles served as the control against which targeted particle deposition profiles are compared.
To illustrate this protocol’s ability to quantify changes in regional pulmonary deposition, data were included for the testing of two different targeting devices: a modified endotracheal (ET) tube (Figure 5B) and a concentric cylinder device (Figure 5E). Both these devices featured a 2 mm ID outlet with tunable location for targeted particle release. The modified ET tube was assessed with the intubated lung model for its ability to target particle deposition to both the Left Lower (LL) Lobe and Right Lower (RL) Lobe. Compared to the non-targeted particle deposition profile, this device generated a nearly four-fold increase in LL Lobe delivery (T-test p=0.004, n=3) in addition to diverting over 96% of delivered particles to the Left Lung (T-test p=0.0001, n=3) (Figure 5A). Altering the release location setting to target the RL Lobe, this device generated more than doubles particle delivery to the RL Lobe (T-test p=0.02, n=3) and diverted 94% of delivered particles to the Right Lung (T-test p=0.0005, n=3) (Figure 5C). This indicates that the device is highly successful in producing the intended deposition profile modulation. The concentric cylinder device was tested in the full lung model with an intended target of the Left Upper (LU) Lobe. Compared to the non-targeted particle deposition profile, this device caused a nearly three-fold increase in LU Lobe delivery (T-test p=0.0003, n=3) in addition to diverting over 87% of delivered particles to the Left Lung (T-test p=0.002, n=3) (Figure 5D). Targeting efficiency can also be observed qualitatively by comparing the images of the target lobe filter to the other outlet filters. As depicted in Figure 3, the most effective targeting method will yield high particle deposition at the intended lobe of interest and low deposition at the remaining lobe outlets. For further demonstrations of the capabilities of this protocol, please see the experiments performed by Kolewe et al9.
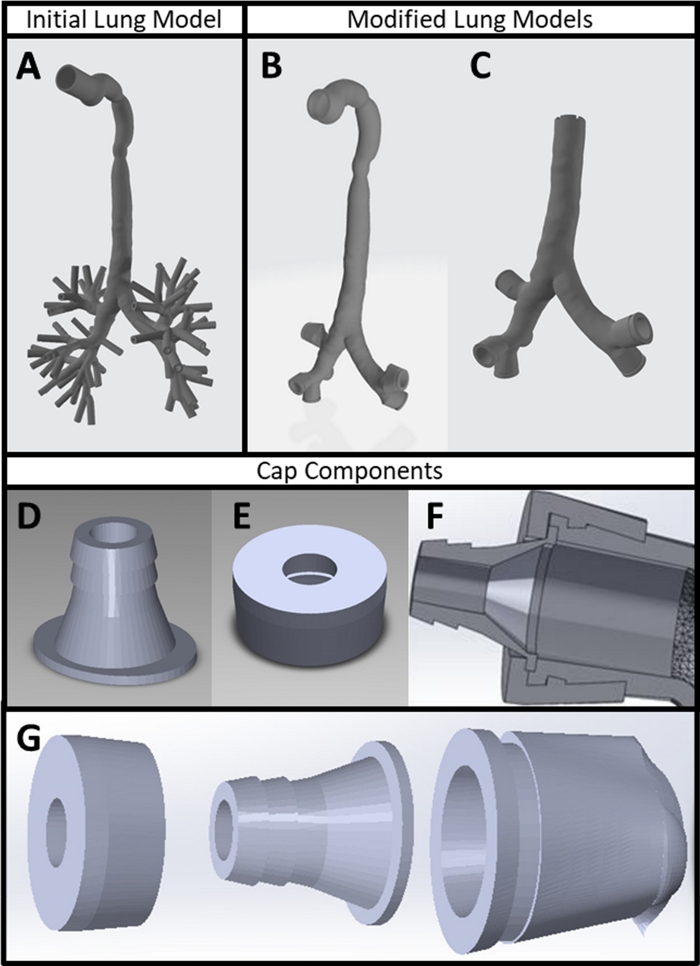
Figure 1: 3D printed experimental components. (A) Patient CT scan converted into 3D part file using CT scan and mesh editing software. (B) Lung model with lobe outlet modifications made in mesh editing and 3D modeling software. (C) Lung model with inlet modified in 3D modeling software to reflect an intubated patient. (D) Barbed tubing connection and (E) cap designed in 3D modeling software. (F) Cross-section of 3D model depicting the interlocking nature of the lung model outlets with the cap and barbed tubing connection. (G) Exploded view of lung model outlet cap assembly. Please click here to view a larger version of this figure.
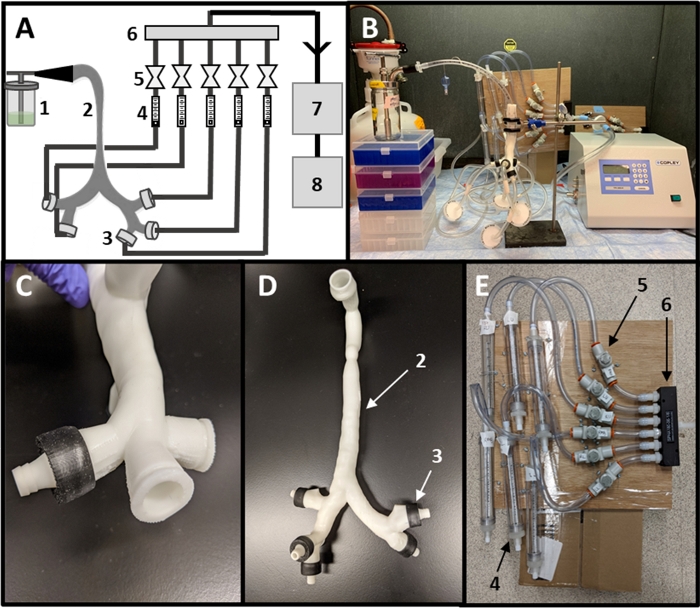
Figure 2: Assembly of experimental setup. (A) Schematic of experimental setup including (1) nebulizer, (2) lung model, (3) outlet caps, (4) flow meters, (5) valves, (6) manifold, (7) flow controller and (8) a vacuum pump. (B) Fully assembled setup. (C) Close-up of lobe outlet with assembled cap. (D) Lung model with all caps added. (E) Close-up of tubing network for setting lobe outlet flow rates. Please click here to view a larger version of this figure.
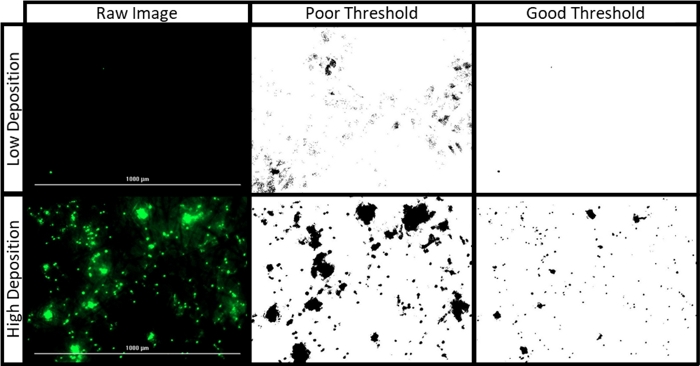
Figure 3: Filter paper image processing. The raw images presented were collected during an experiment to target the left lung using 1 μm fluorescent polystyrene particles at 1 L/min under a healthy breathing profile. The “high” and “low” deposition images depict the LL and RU Lobe filters, respectively. The “good” threshold, applied with a range of 43 to 255, maintains defined edges between individual particles and avoids detection of filter paper fibers. The “poor” threshold, applied with a range of 17 to 255, obscures individual particle borders and overestimates the fluorescent area of the filter. Please click here to view a larger version of this figure.
Figure 4: Experimental setup validation. (A) Validation results for healthy patients and (B) a COPD patient at 1 L/min. All data presented are mean ± SD with three replicates (excepting clinical COPD data, where only one patient was reported). Clinical reference data for healthy and COPD patients were obtained from Sul, et al10. Data sets were compared using Sidak’s Multiple Comparisons Test, and all differences are not significant. Please click here to view a larger version of this figure.
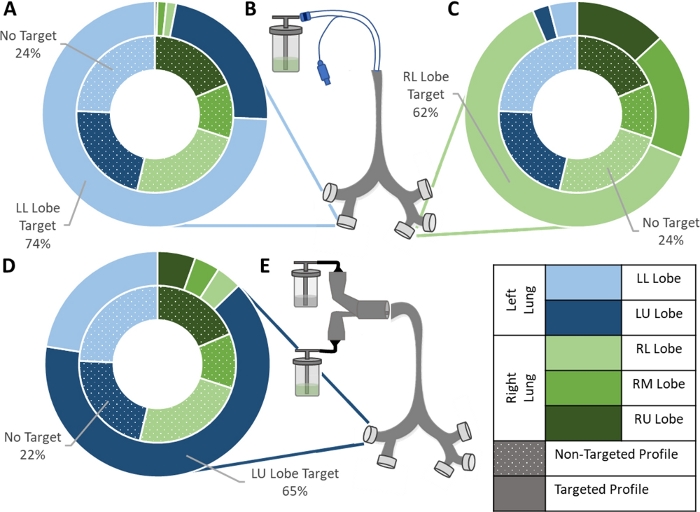
Figure 5: Example data for targeting experiments. (A) Left Lower Lobe and (C) Right Lower Lobe targeting achieved using (B) a modified ET tube delivery system. (D) Left Upper Lobe targeting achieved using (E) a concentric tube delivery system. For all three data sets, the inner ring represents the non-targeted deposition profile obtained during setup validation, and the outer ring represents the deposition profile produced with the addition of the indicated targeting device. Means of three replicates for each setup are shown. Data sets were compared using Sidak’s Multiple Comparisons Test and a Student T-test assuming equal variance. All three setups produced a significant increase in delivery to the lobe of interest: LL Lobe (T-test p=0.004, n=3), RL Lobe (T-test p=0.02, n=3), and LU Lobe (T-test p=0.0003, n=3). Please click here to view a larger version of this figure.