Clinical outcomes
A total of 20 patients underwent OLIF L5-S1 via a retroperitoneal oblique corridor between the Psoas muscle and the great vessels. The study population exhibited female predominance (n=12, 60%), with a mean age of 55.4 ± 6.8 years. OLIF L5-S1 procedures were performed on patients with isthmic spondylolisthesis (n=10), degenerative disc disease (n=6), and degenerative spondylolisthesis (n=4). The procedures included single-level (n=16) and two-level cases (n=4), involving L4-L5 (n=4) and L5-S1 (n=20). The mean blood loss volume was 133.4 ± 48.5 mL, and the average operative time was 153.6 ± 38.3 min. Based on preoperative axial MR images, the left common iliac vein (LCIV) was categorized into three types according to the difficulty of mobilization: type I – no requirement for mobilization; LCIV runs laterally for more than two-thirds of the length of the left side of the L5-S1 disc, type II – easy mobilization; LCIV obstructs the L5-S1 disc space, but the perivascular adipose tissue is present under the LCIV, and type III – potentially difficult mobilization; no perivascular adipose tissue under the LCIV. In our series, patients were classified as type I (n=3), type II (n=14), and type III (n=3) LCIV. For two patients with type III LCIV, no other perioperative complications were observed apart from iliolumbar vein lacerations during exposure.
The preoperative VAS score for lower back pain was 6.3 ± 1.5, significantly decreasing to 1.2 ± 0.8 at 12 months. The VAS score for lower limb pain was 5.6 ± 1.4 preoperatively and significantly decreased to 0.8 ± 0.3 at 12 months (Figure 3). The preoperative Oswestry disability index improved from 82.4% ± 16.2% preoperatively to 8.1% ± 2.0% at 12 months (Figure 4).
Radiographic outcomes
Postoperative radiographic examinations confirmed improved reconstruction at the lumbosacral junction for all patients. At the final follow-up, bony fusion was observed in all patients (Figure 5). No cage retropulsion or pedicle screw loosening cases were observed.
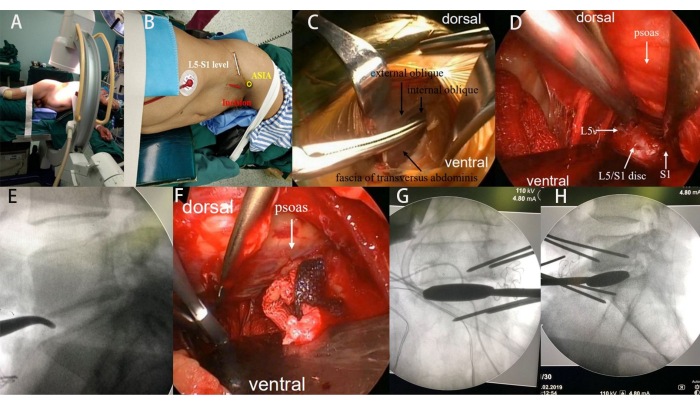
Figure 1: Intraoperative photographs. (A-B) The patient's lateral decubitus position and skin marking for the incision. (C) Blunt dissection involving the external oblique, internal oblique, and transversus abdominis muscles. (D) Exposure of the L5-S1 disc space using handheld retractors and Kirschner wire pins. (E) Intraoperative confirmation of the L5-S1 disc space by fluoroscopy. (F-H) Sequential use of different trial sizes to distract the disc space and release the contralateral annulus. Please click here to view a larger version of this figure.
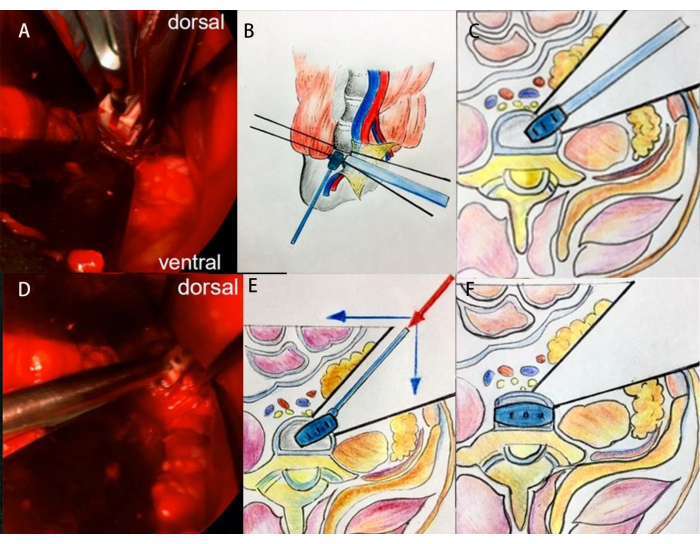
Figure 2: Intraoperative clinical images and schematic diagrams illustrating the technique for cage insertion at the L5-S1 segment. (A-C) First step of cage insertion. (D-F) The second step of cage insertion. Please click here to view a larger version of this figure.
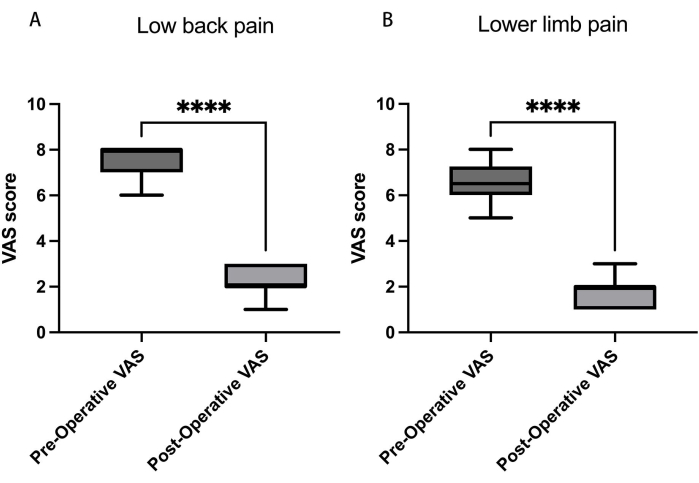
Figure 3: Visual analog scores (VAS) for low back and leg pain. (A) Over 12 months, the VAS score for lower back pain reduced from 6.3 ± 1.5 to 1.2 ± 0.8, and (B) for lower limb pain, the VAS score decreased from 5.6 ± 1.4 preoperatively to 0.8 ± 0.3. Data presented as mean ± SD. ****: Signifies a significant difference by Student's t-tests (p < 0.001). Please click here to view a larger version of this figure.
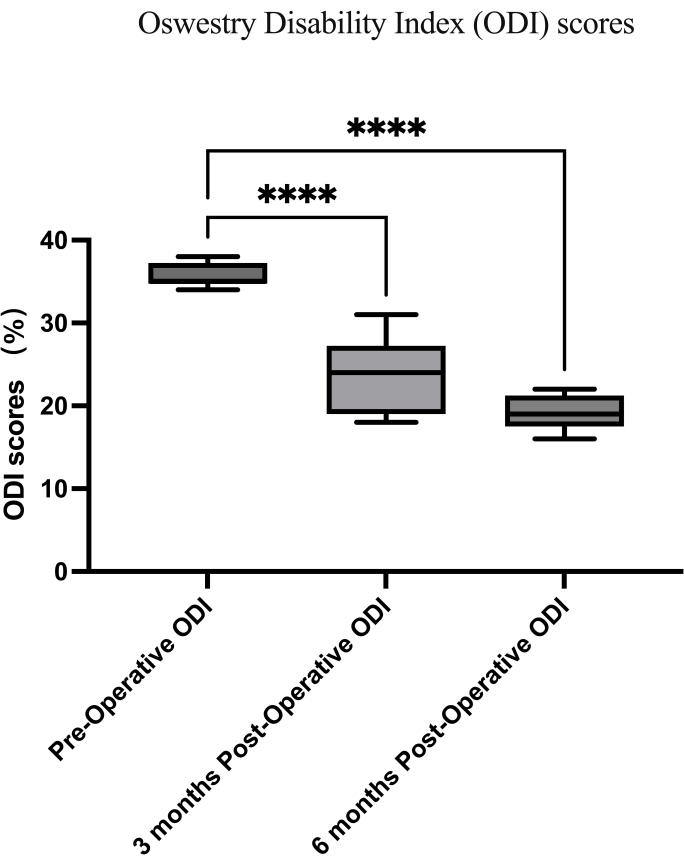
Figure 4: Oswestry disability index scores. The preoperative Oswestry disability index (ODI) improved from 82.4% ± 16.2% to 8.1% ± 2.0% at 12 months. Data presented as mean ± SD. ****: Signifies a significant difference by Student's t-tests (p < 0.001). Please click here to view a larger version of this figure.
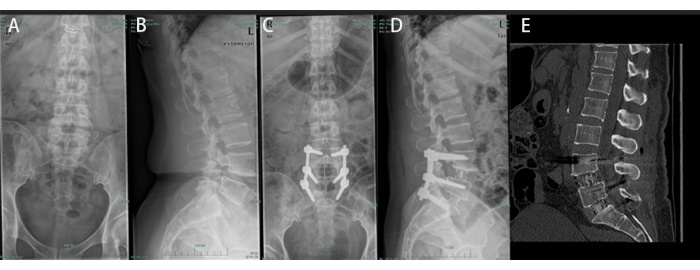
Figure 5: A 51-year-old male undergoing OLIF from L4-5 to L5-S1. (A, B) Preoperative anteroposterior and lateral radiographs displaying spondylolytic spondylolisthesis at L4-L5 and L5-S1. (C, D) Postoperative anteroposterior and lateral radiographs reveal satisfactory L4-S1 reconstruction. (E) Bony union was observed at the final follow-up. Please click here to view a larger version of this figure.