Spine evaluation
Ryan et al. conducted a prospective study to determine the feasibility of rapid spine MRI in the evaluation of syrinx in pediatric patients. Patients with known or suspected syrinx or Chiari malformations underwent rapid spinal MRI (HASTE) and standard non-contrast MR. Images were blindly reviewed by pediatric neuroradiologists who measured the following outcomes: Presence or absence of syrinx, syrinx measurement, clonus position, cerebellar tonsillar ectopia and degree, and filum detection. They identified syrinx (sensitivity 87.8%, specificity 94.7%) if greater than 2.3 mm in size and if the patient was older than 1 year old. There was no clinically significant difference between spinal rapid MRI and standard spinal imaging9. An example of a lumbosacral syrinx identified by RS-MRI can be seen in Figure 2.
Gewirtz et al. conducted a retrospective chart review of patients who underwent spinal rapid MRI. Patients' (n = 45) scans were reviewed and compared with radiographic reports and clinical notes, and 47 scans were included in the analysis. Clinical indications for scan included syrinx (n = 30) and spinal dysraphism (n = 22) evaluation. All 47 scans were interpretable and usable (n = 8 moderate motion artifacts). Subsequent standard MRI follow-up scans (n =7) were completed within 1 year, and no new abnormalities were detected10.
Traumatic brain injury evaluation
Lindberg et al. conducted a prospective cohort study where they attempted RS-MRI in children <6 years old who had a prior head CT. The primary outcomes were feasibility and accuracy. Feasibility was measured by RS-MRI completion rate and imaging time. Accuracy was measured against CT and was assessed by the ability of the RS-MRI to identify skull fracture, intracranial hemorrhage, and parenchymal injury. A total of 223 RS-MRIs were conducted with a median imaging time of 365 s. Of the 111 patients identified with TBI on CT, RS-MRI detected 103 of these (sensitivity 92.8%, 95% confidence interval 86.3-96.3). RS-MRI failed to detect 6 isolated skull fractures and 2 subarachnoid hemorrhages. These findings concluded that RS-MRI is feasible and accurate relative to CT in clinically stable patients5.
Kessler et al. conducted a systematic review of the use of RS-MRI in the setting of pediatric head trauma. A total of 13 articles were identified and reviewed. In addition to the Lindberg article listed above, they reviewed Kralik et al., Missios et al., and Sheridan et al., which were a combination of retrospective and prospective studies of multisequence MRI. These four studies concluded that RS-MRI can be used without concurrent imaging modalities. Additional studies that utilized RS-MRI with tri-planar T2-weighted imaging alone were reviewed and compared to concurrent HCT or standard brain MRI. The sensitivity and specificity of RS-MRI were 100% and 97% for the detection of IPH, 86% and 96% for extra-axial hemorrhage, 10% and 100% for SAH, 50% and 100% for IVH, and 47% and 97% for skull fractures respectively. Further, Ryan et al. discussed the decreased sensitivity of RS-MRI to skull fractures, noting that only 11 of the 41 fractures were detected. The articles reviewing the utilization of the T2 sequence only concluded that across all pathologies, the sensitivity to TBI pathology was increased when used concurrently with HCT. To address the poor detection of skull fractures by RS-MRI, an article by Dremmen et al. was reviewed, which included the novel black bone sequence to T1-weighted imaging and determined that RS-MRI had a sensitivity and specificity of 66.7% for detected skull fracture. Of those skull fractures, there were 2 false negatives and 2 false positives. The false positives were later noted to be sutures and the patient population most affected by these findings were children under 2 years old. Lastly, a conglomerate of articles was reviewed where RS-MRI alone was compared to matched cohorts who received standard imaging (HCT/standard brain MRI). Cohen et al. found that more radiographic abnormalities were found in the HCT group, and those patients were, on average, triaged at higher levels of care. From this systematic review, Kessler et al. concluded that RS-MRI is a promising option when compared with HCT and standard MRI but may be less sensitive to traumatic pathology and that appropriate imaging modalities should be selected in the clinical and institutional context1.
Ryan et al. examined the ability of RS-MRI T2 sequences to detect intracranial hemorrhage. Patients who presented to the pediatric hospital with acute intracranial hemorrhage on CT had a follow-up RS-MRI 48 h later, and the two imaging modalities were compared. RS-MRI had modest sensitivity to detect subdural and epidural hemorrhages in the absence of prior CT; sensitivity ranged from 61%-74% but increased to 80%-86% with the review of the prior CT. The addition of GRE sequences to standard T2 sequences increased the sensitivity of detecting subarachnoid hemorrhage from 10%-25% to 71%-93%. Ryan et al. included that RS-MRI with GRE is most sensitive for detecting intracranial hemorrhages when prior CT is available and is not adequate to replace CT in the initial evaluation6. A T2 Haste from RS-MRI showcasing right extra-axial hemorrhage along right cerebral convexity is shown in Figure 3.
Hydrocephalus and shunt evaluation
A retrospective chart review conducted by O'Neill et al. included patients who underwent RS-MRI and compared that to prior HCT. The median age was 1.3 years. Patients underwent an average of 2.38 RS-MRI and 10.1 HCTs. All RS-MRIs were reviewed by a radiologist and blinded neurosurgeon, and image quality and catheter visualization were graded. Secondary outcomes were the amount of motion artifact and ventricular size. The radiologist rated 51.2% of RS-MRIs as having excellent imaging quality compared to the 76.5% rated by the neurosurgeon. Further, there were differences in catheter visualization by radiologists (24.4%) when compared to neurosurgeons (42.9%), and visualization was most problematic in the setting of small ventricles. It was concluded that axial RS-MRI provides good visualization of ventricular anatomy with the risk of potential valve failure11. An example of this can be seen in Figure 4, which demonstrates a sagittal view of a shunt catheter (Figure 4A) and an axial view showcasing ventriculomegaly (Figure 4B).
Yue et al. conducted a two-site retrospective chart review to compare RS MRI vs non-contrast CT in the evaluation of shunt malfunction of pediatric patients who presented to the ED. Shunt malfunction was defined as necessary neurosurgical shunt revision within 30 days of initial imaging. There were 997 scans used in the analysis (RS-MRI= 724, CT=273). There was a total of 235 shunt revisions (RS-MRI= 188, CT= 47). The sensitivity to detect shunt malfunction in the RS-MRI group was 58.5% (95% CI 51.1%-65.6%), and the specificity was 93.3% (95% CI 90.8%-95.3%). In the CT group, the sensitivity to detect shunt malfunction was 53.2% (95% CI 38.1%-67.9%), and specificity was 95.6% (95% CI 92%-97.9%). It was found that there was no statistically significant difference between sensitivity (p=0.51) or specificity (p=0.23)12.
Boyle et al. conducted a single-center retrospective chart review of pediatric patients who presented to Boston's Children's ED with concerns about shunt malfunction to determine the diagnostic accuracy between rapid cranial MRI and CT to diagnose ventricular shunt malfunction. Shunt malfunction was defined as the need for surgical intervention due to mechanical shunt flow alterations within 72 h of initial ED evaluation. The noninferiority test of the accuracy of rapid cranial to CT for diagnosing shunt malfunction, with a noninferiority margin of 10%, was used as the primary analysis. A total of 698 ED visits were included in the analysis (between 286 patients), of which patients received rapid cranial MRI scans (n = 362) and CT scans (n = 336). ED visits (n = 140) resulted in shunt revision. The accuracy of RS-MRI was similar to that of CT scans for diagnosing ventricular shunt malfunction (81.8% MRI vs. 82.4% CT), with an increase in RS-MRI use over the study period. Neurosurgical attending and neuroimaging modality were positively correlated (χ2 = 93.9, P < .001)13.
Boyle and Nigrovic reviewed the literature to compare the different neuroimaging modalities used to diagnose shunt malfunction in pediatric patients in the emergent setting. A review of the literature concludes rapid cranial MRI is an alternative non-inferior modality compared to CT when diagnosing shunt revision in children14. Table 2 showcases a summary of the representative results and their conclusions1,5,6,9,10,11,12,13,14.
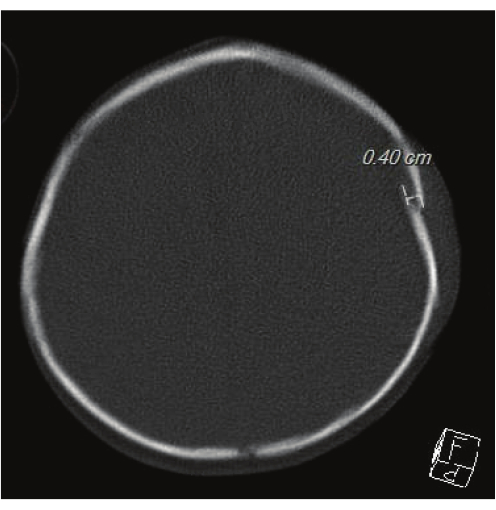
Figure 1: Head CT for evaluating skull fractures. This image showcases the gold standard Head CT. A 0.40 cm left parietal fracture can be seen. Please click here to view a larger version of this figure.
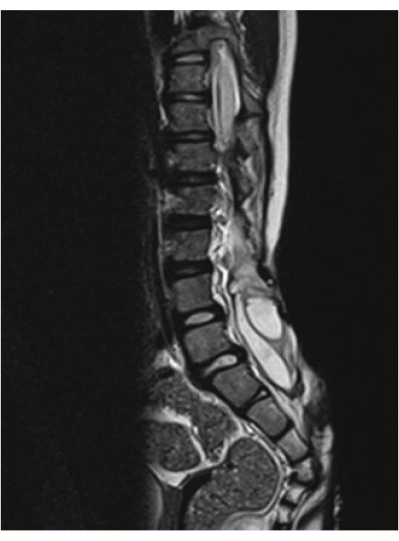
Figure 2: T2 spinal imaging showcasing syrinx. The image showcases a lumbosacral syrinx that is identified by RS-MRI. Please click here to view a larger version of this figure.
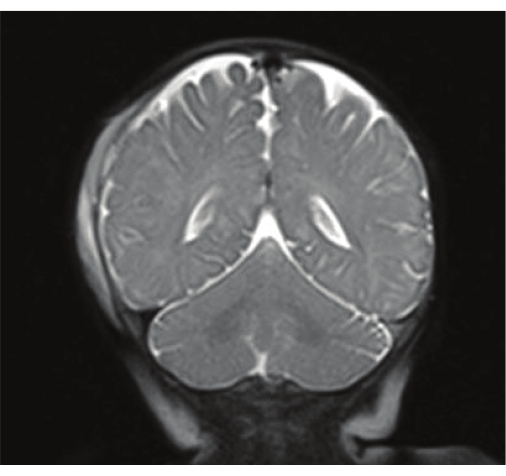
Figure 3: TBI findings from RS-MRI. The image is a T2 Haste from RS-MRI showcasing right extra-axial hemorrhage along right cerebral convexity. Please click here to view a larger version of this figure.
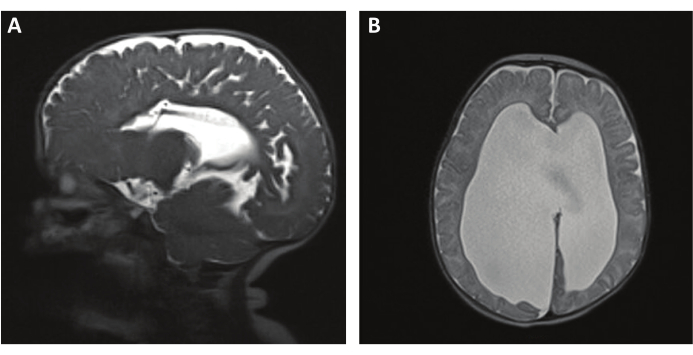
Figure 4: RS-MRI T2 HASTE for shunt evaluation and ventriculomegaly. (A) A T2 HASTE sequence showing a sagittal view of a shunt catheter. (B) An axial T2 HASTE image showing ventriculomegaly. Please click here to view a larger version of this figure.
Table 1: Summary of RS-MRI sequences for CNS pathology. The table provides a summary of recommended MRI sequences from the combined protocols above. BB= black bone Please click here to download this Table.
Table 2: Summary of representative results. The table provides a summary of the representative results showcasing the study type, comparative sequences, sensitivity and specificity, and conclusions. Please click here to download this Table.