A retrospective study of patients with Achilles tendinopathy was performed on individuals older than 18 years old, with a definite diagnosis of Achilles tendinopathy. Exclusion criteria were recent ankle surgery or any condition that is a contraindication of ESWT.
This study included 36 participants. diagnosis with Achilles tendinopathy, 18 females and 18 males. Of these patients, their average age was 43.7 years, ranging between 18 and 64 years. All the patients complained of pain; 11 out of 36 patients had reduced range of motion (Table 1).
The treatment protocol was applied to all participants. In our study, the minimum number of sessions was one, and the maximum was eight. For these participants, a significant decrease in pain was achieved, and 4 of them were even pain-free after treatment, although all of them complained of pain at the beginning. Only 4 of them had impairment of ankle range of motion at the end. They got a significant improvement in the VISA-A Scale, which increased from 50.3 to 90.5.
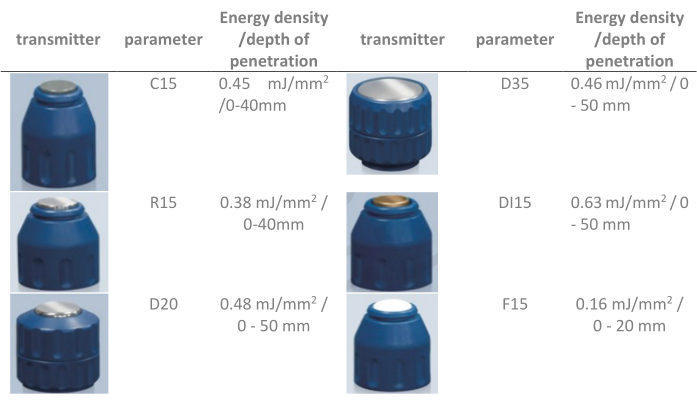
Figure 1: Illustrations of six different transmitters and their specifications. Please click here to view a larger version of this figure.

Figure 2: Applicator positioning. Please click here to view a larger version of this figure.
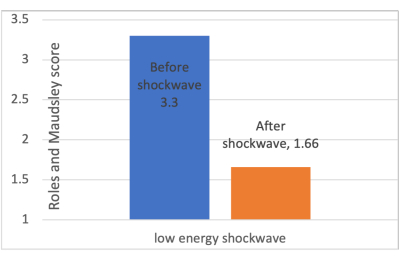
Figure 3: Changes in Roles and Maudsley scores before and after low-energy ESWT. The Roles and Maudsley scale allows the patient to subjectively describe their pain, with a score ranging from 0 to 4 points from excellent to poor. Abbreviation: ESWT = extracorporeal shockwave therapy. Please click here to view a larger version of this figure.
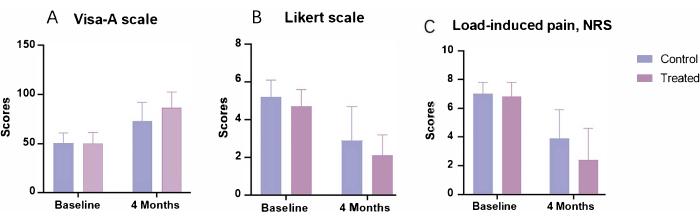
Figure 4: Changes in primary outcome measures before and after the 4 month follow-up. (A) The Victorian Institute of Sport Assessment-Achilles Scale used to evaluate the clinical severity of patients with chronic Achilles tendinopathy, had a maximum score of 100. (B) The Likert scale, used for general assessment, was scored by the patient on a 6 point scale (1 = completely recovered, 2 = much improved, 3 = somewhat improved, 4 = hardly improved, 5 = not improved, 6 = worse). (C) Numeric Rating Scale used to assess pain severity when patients with Achilles tendinopathy load, using a 0-10 scale. The control group received a 12 week eccentric exercise program, and the treated group received the same exercise protocol combined with three sessions of radial-ESWT treatment. Abbreviations: ESWT = extracorporeal shockwave therapy; VISA-A = Victorian Institute of Sport Assessment-Achilles; NRS = Numeric Rating Scale. Please click here to view a larger version of this figure.
| Demographic characteristics | ||
| Age | 43.7(18-64) | |
| Gender | Male | 18(50%) |
| Female | 18(50%) | |
| Number of sessions | 2.58(1-8) | |
| Visual Analogue Scale(VAS) | Before | 4.06(3-5) |
| After | 1.28(0-3) | |
| Stiffness | Before | 11(30.5%) |
| After | 4(11.1%) | |
| Complications | 10(27.8) | |
Table 1: Demographic characteristics. Visual Analogue Scale used Numerical rating scales with 0-10 scores; a higher score indicates greater pain intensity. Abbreviation: VAS = Visual Analogue Scale.
| Authors | N. partici-pants | Follow-up (months) | Treatment | Parameters | outcome measures (pain) | Functional improvement | |||||
| Rompe et al. 24 | 68 | 4 | eccentric loading vs eccentric loading + low-energy ESWT | radial ESWT, 2000 shocks, 3 Bar | VAS –13.5 (–22.5 to 5.5) ( P = .0016) |
Likert scale 0.8 (0.08 to 1.5), P = .035 |
|||||
| Pavone et al.26 | 40 | 12 | ESWT + eccentric exercises | Low-energy radial ESWT, 4 sessions, 800 shocks, 4 Hz | VAS −5.8 ± 1.2 SD (P < 0.001) |
AOFAS +19.8 ±5.0 SD (P < 0.001) |
|||||
| Saxena et al.27 | 60 | 12 | ESWT | low-intensity 2500 shocks, at 2.4 Bar ranging, 11 to 13 Hz | / | Roles-Maudsley 1.44 ± 0.87 SD (P < 0.001) |
|||||
| Vahdatpour et al.28 | 43 | 4 | ESWT vs Sham SWT | 1500 shocks, focused shockwaves (0.25–0.4 mJ/mm2, 2.3 Hz); 3000 shocks, radial shockwaves (1.8–2.6 mJ/mm2, 2.21 Hz). | VAS. −3.70±2.27 (p<0.001) | AOFAS 20.90±13.51, p<0.001 |
|||||
| Wheeler et al.29 | 39 | 6 | ESWT | 10 Hz and 2000 shocks | painDETECT questionnaire. −4.8 (NAT) and −3.9 (IAT) (P < 0.01) |
VISA-A 23% (0% to 43%)(IAT) and 11% (7% to 22%)(NAT) |
|||||
| Taylor et al.30 | 54 | 24 | ESWT | Low-energy radial ESWT, 2000 shots, 10 Hz, 1.5–2.5 bar | VAS −4.8 (NAT) and −3.9 (IAT) (P < 0.01) |
VISA-A +66 points (P < 0.001) |
|||||
Table 2: Case series and primary outcome measures after treatment. Abbreviations: SWT = shockwave therapy; ESWT = extracorporeal SWT; VAS = Visual Analogue Scale; NAT = Non-insertional Achilles tendinopathy; IAT = Insertional Achilles tendinopathy; VISA-A = Victorian Institute of Sport Assessment-Achilles; NRS = Numeric Rating Scale; AOFAS = American Orthopedic Foot and Ankle Society.
