The US-guided injection is an effective technique to obtain real-time and precise needle visualization for BoNT administration in the salivary glands. This approach provides a reliable sialorrhea treatment, with prolonged efficacy and the absence of serious adverse events. Indeed, the visualization of the glands and of the needle penetration provided by the US-guided approach proposed here allows a widespread administration of BoNT-A within the major salivary glands with significant and long-lasting outcomes. Sialorrhea reduction can be easily observed 1 w after the treatment through the administration of the DFSS and VAS and through the collection of the number of daily aspirations through a saliva aspirator (if appropriate). These data allow a quick follow-up assessment and are useful to evaluate the need for retreatment. We recommend patients for another BoNT-A injection when the number of daily aspirations increases to over 50% of the best efficacy obtained after the previous injection (obtained about 1 month after the treatment). This technique usually allows a treatment interval of 6 months and leads to a significant reduction in severity and frequency of sialorrhea, with a decrease of about 50% in the DFSS. In detail, the DFSS severity score showed a significant reduction from the pretreatment average score of 4.06 ± 0.81 to the average 1-month post-treatment score of 1.73 ± 1.65, and the DFSS frequency score reduced from the pretreatment average of 3.46 ± 0.75 to the average 1-month post-treatment of 1.82 ± 0.56. The VAS score changed from the pretreatment average of 3.01 ± 1.21 to the average 1-month post-treatment of 8.33 ± 1.10. Finally, the need of daily saliva aspirations lowered from the pretreatment number of 11.90 ± .88 to the 1-month post-treatment number of 4.44 ± 1.43. On average, sialorrhea improvement can be observed as soon as 1 w after injection (Figure 3a, b, c, d).
The US identification of the different tissues and of the needle route also provides an important reduction in adverse events, avoiding BoNT injection into incorrect targets and needle penetration through neurovascular structures. The most common adverse events observed with this technique are mild and consist local pain, dry mouth, viscous saliva, and local bleeding7,13,15.
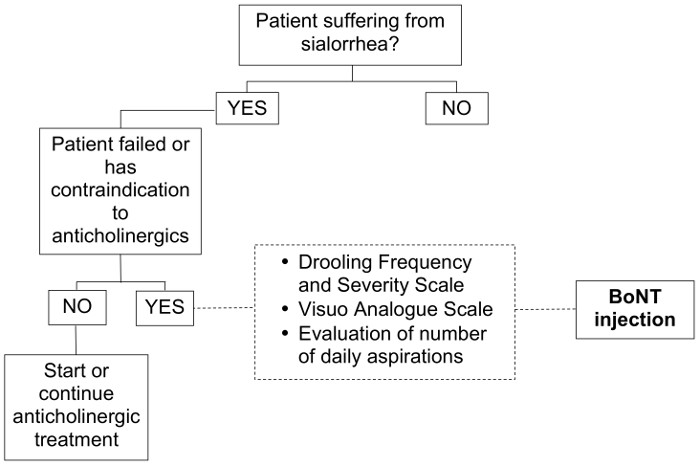
Figure 1: Flow-chart of Patient Selection. Patient evaluation and selection for BoNT-A treatment. Please click here to view a larger version of this figure.
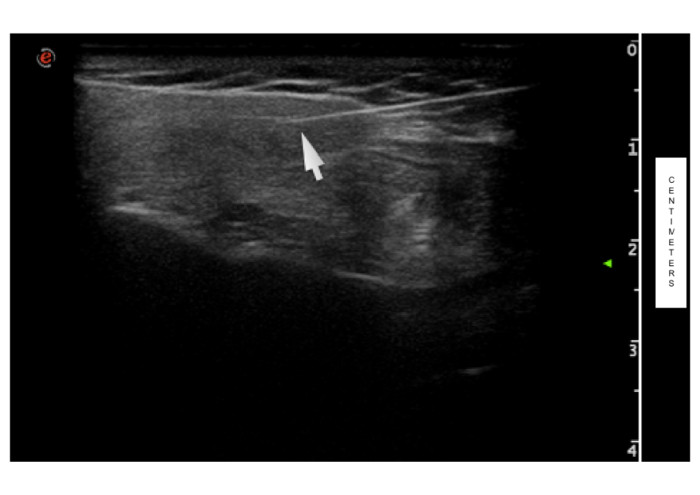
Figure 2: Ultrasound Injection of Parotid Gland. The arrow indicates the needle penetration, visible as a bright echoic line, within the parotid glandular tissue. Unit scale is expressed in cm. Please click here to view a larger version of this figure.
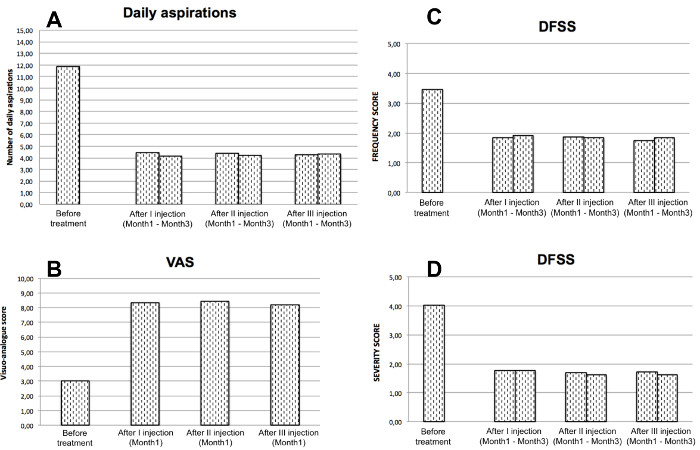
Figure 3: Clinical Outcome of BoNT-A Treatment. Pre = evaluation before therapy; post = evaluation 1 month after therapy; DA = number of Daily Aspirations; VAS = Visual Analogue Scale; FS = Drooling Frequency and Severity Scale – frequency subscore; SS = Drooling Frequency and Severity Scale – severity subscore. Please click here to view a larger version of this figure.
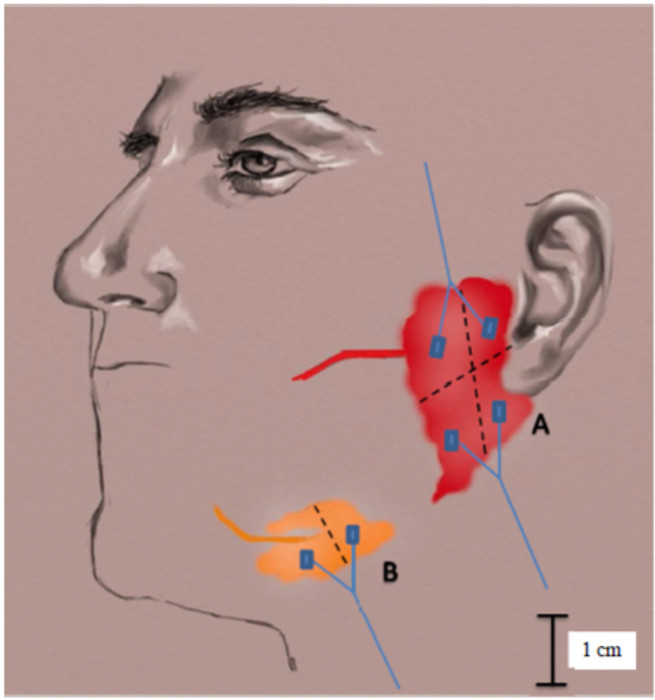
Supplemental Figure: Representation of the Ideal Injection Sites. A) Schematic division of the parotid gland into four quadrants, two cranial and two caudal, for correct injection into four different glandular sites. B) Schematic division of the submandibular gland into one cranial and one caudal quadrant for correct injection into two different glandular sites.
