The protocol was approved by the University of Leuven Ethical Review Board for Animal Research.
1. Preparation of the Venous Line
- Prepare the tip of the venous catheter by quickly immersing the middle part of 60 cm microrenathane (MRE) tubing in hot (> 220 °C) sesame oil. Subsequently stretch the middle part of the tube to produce a narrow diameter (outer diameter (OD) < 0.5 mm) by gently moving the ends of the tubing away from each other.
- Use a scalpel blade to cut the tubing into two parts of 30 cm each (see Figure 1, Table 1).
- Connect the MRE tubing to polyethylene tubing PE10 using polyethylene PE50 connector and connect this PE10 tubing to the bottom part of the swivel. Connect the upper part of the swivel to PE10 tubing, and connect this to a Luer stub needle with PE50 connector tubing as per Figure 1.
- Apply strong fast-acting adhesive glue to all connections and test the catheter for leakage by flushing with air. Gas sterilize the catheter prior to use.
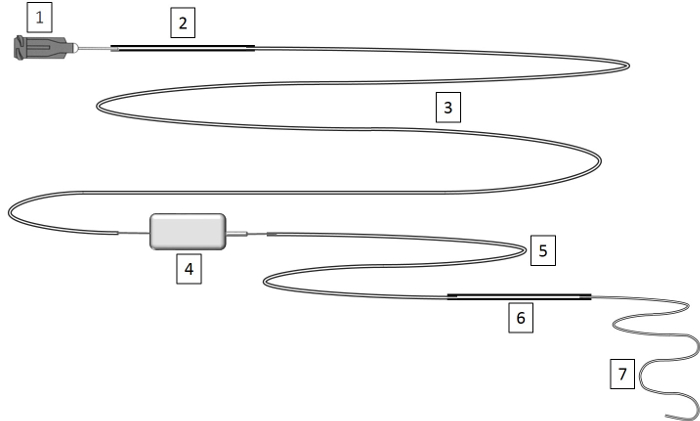
Figure 1: Construction of Venous Line. Venous lines are prepared by stretching the MRE tubing to a small diameter and connecting it via polyethylene tubing to a rodent swivel device. See Table 1 for instructions on lengths of the different parts. Please click here to view a larger version of this figure.
| Legend | Length | Volume |
| 1) Luer stub needle 22 G | ||
| 2) PE50 – polyethylene .023" x .038" | 5 cm | 13 µL |
| 3) PE10 – polyethylene .011" x .024” | 50 cm | 30 µL |
| 4) Rodent Swivel 20 G | ||
| 5) PE-10 | 15 cm | 9 µL |
| 6) PE-50 (connector) | 5 cm | 13 µL |
| 7) MRE025 Tip stretched microrenathane .025" x .012" | 30 cm | 27 µL |
| Total sum | 105 cm | 92 µL |
Table 1: Construction of Venous Line. This table provides a legend for Figure 1.
2. Anesthesia and Pre-surgery Handling
- Use 24-week old male C57BL/6J mice (27 – 32 g).
NOTE: We use 24-weeks-old mice (mature adult) as this age corresponds better with the mean age of intensive care patients. We use only male mice to avoid the cyclic influence of estrogens. The technique can also be used on younger animals (tested in 16-week old mice) and females, if preferred. - Sterilize all surgical instruments before use. Flush the sterile home-made venous catheter with saline to remove any air bubbles and to test for patency and potential leaks.
- Cut a metal wire (0.8 mm diameter) of 80 cm length, double it by folding and make a loop. Lead 3 pearls over the doubled wire to the loop. Attach the catheter to the metal wire by guiding the tip of the catheter through the 3 pearls.
NOTE: The metal attachment wire is necessary for rotation of the swivel to which the catheter is connected. As such, the mouse can move freely, without blocking the venous line. - Anesthetize the mouse by an intraperitoneal (IP) injection of a mixture of 0.03 mL ketamine (100 mg/kg) and 0.02 mL xylazine (13 mg/kg). Ensure that anesthesia is adequate by checking the absence of reflexes. Gently pull the mouse tongue outside with forceps to avoid suffocation by swallowing of the tongue.
NOTE: If after 10 min, the mouse still attempts to withdraw its limbs give additional ketamine as a 0.01 mL bolus. - Shave the surgical area including abdomen, ventral side of the neck (triangle between chin, sternum and clavicle), and between shoulder blades at the base of the head).
- Place the mouse in prone position on a pre-warmed heating pad, disinfect the skin with 70% ethanol and apply a small amount of ophthalmic lubricant to protect eyes from drying out. Infiltrate the surgical sites (abdomen, neck-front and back) with 0.2 mL ropivacaine (0.67 mg/kg).
- While the mouse is still in prone position, make a small incision at the base of the dorsal side of the head with scalpel or scissors. Expose the posterior cervical muscles, and tie the muscle to the loop of the attachment wire with 3.0 nylon by leading a 3.0 nylon thread under the muscle.
- Place the mouse on its right side. Make a small vertical incision in the skin of the ventral neck with a scalpel or scissors. Under visual guidance, tunnel an 18-gauge needle subcutaneously through this ventral incision towards the incision on the back made previously and thread the catheter through the needle to exteriorize it at the ventral side.
- Place the mouse on its back. Pass a 3.0 nylon thread behind the top incisor teeth of the mouse and tape it down to the heating pad. Secure the head in a face mask for delivering oxygen (2 L/min). Fix the mouse in a stretched position by taping down the tail and the two forelimbs.
NOTE: If the ketamine-xylazine anesthesia alone is not sufficient, inhaled isoflurane (0.5 – 1.5%) can be delivered during surgery.
3. Placement of a Chronic Indwelling Catheter
- Place the mouse under the dissecting microscope. In the incision made previously in the ventral neck, gently tease fat tissue and glands away with forceps until the jugular vein can be visualized.
- Bluntly dissect to free the jugular vein from the connective and subcutaneous tissue above and around the vessel by placing the tip of the forceps between the vein and connective tissue and opening the forceps repeatedly in parallel with the vein. As such, damage to the vein will be avoided.
- Isolate the jugular vein by placing blunt forceps under the vein. Feed three pieces of 3.0 silk thread under the vein, position one piece proximal to the bifurcation of the jugular vein (cranial ligature) and one piece close to the sternocleidomastoid muscle (caudal ligature). Tighten the cranial ligature and the caudal ligature to stretch the vein and prevent excessive bleeding while placing the catheter. Tie a loose ligature with the middle thread to ensure easy securing of the catheter later on.
- Using micro scissors, make an incision along the vein between the cranial and caudal ligatures and large enough to pass the catheter. Grab the catheter with forceps, and insert the catheter 11 mm into the vein. Loosely secure the catheter by tying off the middle ligature and confirm correct placement by gently flushing with sterile saline.
- Secure the catheter by firmly tying off the middle and caudal ligature around the vessel and catheter. Tie ends of caudal and middle ligature together to firmly secure the catheter. Ensure that the knots do not occlude the vein, by flushing the catheter after every knot made. Finally, tie the caudal and cranial ligatures. Close the incision with 5.0 silk sutures.
4. Cecal Ligation and Puncture
- Make a 1-cm midline incision through skin of the lower half of the abdomen with scalpel or scissors; be careful not to penetrate into the peritoneal cavity.
- Identify the linea alba of the abdominal musculature and make an intermuscular incision to gain entry into the peritoneal cavity. Locate the cecum, and use blunt anatomical forceps to isolate the cecum and exteriorize it.
- Ligate the cecum at 50% of its length with 3.0 silk sutures. Make sure not to ligate the ileocecal valve so that intestinal continuity is maintained.
- Perforate the cecum with an 18-gauge needle by a single through-and-through puncture midway between the ligation and the tip of the cecum. After removing the needle, extrude a small amount of feces from the hole to ensure patency.
- Reposition the bowel in the abdominal cavity, and close the peritoneum and skin with 5.0 silk sutures.
NOTE: On average, a new trainee requires 10 to 15 animals to be able to smoothly place the venous catheter and perform CLP within 45 min. After the training period, an anesthesia/surgery related mortality of 10% can be expected.
5. Post-surgical Treatment and Fluid Resuscitation
- Place the mouse in supine position and secure the catheter to the attachment wire with tape. Move the mouse to an individual cage. Use a stand with adjustable clamp to hold the swivel device 25 cm above the mouse and firmly tape the free part of the metal attachment wire to the rotating point of the swivel.
- Attach a syringe containing the mixture of balanced colloids and crystalloids (1:4) to the venous line to start fluid resuscitation.
- Place the cage in a temperature controlled (27 °C) animal cabinet with 12 h light and dark cycles and start intravenous fluid resuscitation (10 mL/kg/h) via an accurate syringe-driven infusion pump. Provide cage enrichment such as nesting material and a wooden block.
6. Intensive Care
- At 6 h post-operation, subcutaneously inject pain medication and antibiotics (0.3 mL buprenorphine (0.15 mg/kg) and 0.2 mL imipenem (16.67mg/kg)). NOTE: Following standard laboratory animal medicine practice, the first dose of pain meds is given prior to the initial surgical incision and then as directed by the institution’s veterinary policies. Subcutaneous injections should be carefully injected into the subcutaneous space.
- After 20 – 24 h of fluid resuscitation, replace the crystalloids/colloids by total parenteral nutrition (6.67 mL/kg/h).
NOTE: Total parenteral nutrition administered (5.8 kcal/24 h) covers around 40% of the daily caloric needs of mice, similar to the early caloric intake of patients in the intensive care unit. - Subcutaneously administer pain medication and antibiotics (0.6 mL buprenorphine (0.3 mg/kg) and 0.2 mL imipenem (16.67 mg/kg) every 12 h during the whole period of critical illness.
- Check the animals at least every 3 h during the day. Assess suffering by giving a pain score based on the validated mouse grimace scale11. Intensify monitoring for animals with a high pain score.
7. End of the Experiment
NOTE: Approval of and recommendations on the level of severity of the model and guidelines and policies for human endpoints should be sought from the local Institutional Ethical Review Board for Animal Research.
NOTE: In case of a nonfunctional venous line such as blocked catheter, delocalization of the catheter, problems with the syringe pump, the animal is excluded from the study and euthanized.
- At the end of the experimental period, deeply anesthetize the mouse using a mixture of 0.03 mL ketamine (100 mg/kg) and 0.02 mL (13 mg/kg) xylazine. Euthanize the mouse by withdrawing blood by cardiac puncture. Store snap frozen tissue samples of interest at -80 °C.
C57BL/6 mice were made critically ill as described above. We performed two experiments to assess post-CLP survival until two time points: survival until day 5 (n = 15) and survival until day 7 (n = 22) post-CLP. Survival curves of the two experiments were not significantly different (compared until day 5), indicating the reproducibility of the experimental setup. Non–surviving animals were found death or euthanized due to reaching human endpoints. Ligation of 50% of the cecum in combination with antibiotics, fluid resuscitation and total parenteral nutrition via a venous catheter in the vena jugularis, as described, resulted in a 13% mortality after 1 day of critical illness, 24% mortality after 3 days of critical illness, 27 – 31% mortality after 5 days of critical illness and 36 % after 7 days of critical illness. The healthy pair-fed mice, which were caloric restricted to the nutrient intake of the critically ill mice, did not show any mortality.
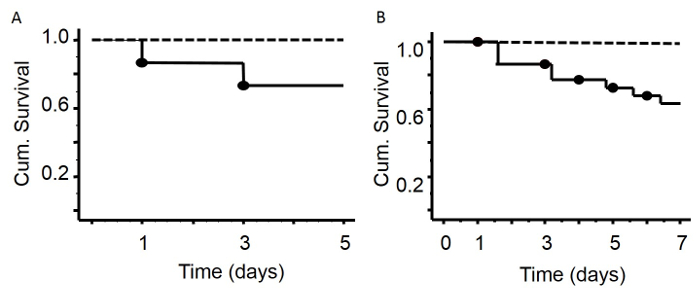
Figure 2: Survival Curves after 5 or 7 Days of Critical Illness. There was no mortality in the group of healthy animals (A, B, dashed line – healthy animals without surgery). Five days after surgery (A), mortality rate was 27% (solid line). Seven days after induction of sepsis (B), the mortality rate was 36%. Mice with leaking or dislodged catheters were excluded from the experiment (15%). Please click here to view a larger version of this figure.
