Histological analyses revealed that the harvested tissue from lateral epicondylitis had the characteristics of a tendinopathic tendon.H&E section of tendinopathy degenerative tendon revealed a disorganized collagen bundle with a loss of polarity and fine straight, strongly packed parallel fiber structures. Histological signs suggestive of degeneration such as higher cellularity and enlarged nuclei without the typical spindle shape were common in samples. Additionally, collagen bundles of the degenerated tendon were relatively weak eosin stained by H&E but were positively stained by Alcian blue indicating increased proteoglycans and glycosaminoglycans substance.
In all cases, blood vessels were increased in number and aggregates occupying spaces embedded between fibers were compared to normal slit-like blood vessels. In the IHC staining, cells of degenerated tendons showed cytoplasmic granular positive reaction to VEGF in comparison to the negative reaction of control ones. Collectively, these findings confirmed that the harvested tissues from lateral epicondylitis were degenerative tissues and suitable for the degenerative tenocyte culture (see Figure 2).
The cultured cells were confirmed as tenocytes by ICC and the harvested tissues were confirmed by IHC as tendon tissue. Most of the cultured cells and cells in tendon tissue showed a positive stain for the representative tenocyte markers known as mohawk (green) proteins and tenomodulin (red) proteins with an elongated appearance under microscopy (see Figure 3). Also, the harvested tissues had the positive staining for mohawk proteins and tenomodulin proteins immunohistochemically (see Supplementary Figure 1). These suggested that the harvested tissues were composed by the tendon tissue.
Cultured tenocytes from the harvested tissue of lateral epicondylitis had the characteristic features that correspond to tendinopathy. Both degenerative and healthy tenocytes were cultured for 4 days under the same condition. At each time point, the proliferation rate was measured by BrdU assay and WST-1 assay. The results showed that the proliferation rate of the degenerative cells was significantly higher compared to the controls as previously reported (p <0.05) (see Figure 4A).
Five genes which are known to be up-regulated in the degenerative tendon were analyzed by qRT-PCR. Expressions of the genes, COL3A1, ACTA2, TAC1 (SP), TAC receptor 1, and PTGS2 (COX2) were increased more significantly in the cultured cells from the degenerative tendon than in the cells from the healthy ones. The relative expressions for all genes are shown in Figure 4B and Supplemental Figure 2.
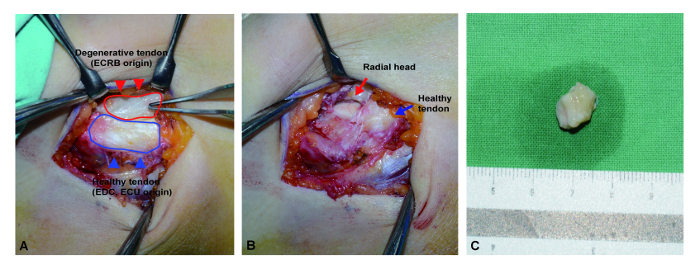
Figure 1: Surgical photo of degenerative tendon harvest. (A) After skin incision and dissection, the pathologic degenerative tissue on the common extensor origin was exposed, showing a characteristic dull-grayish color with edematous change (red line). Conversely, the general appearance of normal tendon tissue was shiny and firm with a slightly grayish tone (black line). (B) All identified degenerative tissues were resected sharply and then the radial head bone was exposed. (C) All resected tissues were embedded into the phosphate buffered saline immediately and the surrounding non-tendinous tissue was carefully dissected as soon as possible. ECRB: extensor carpi radialis brevis. EDC: extensor digitorum communis. ECU: extensor carpi ulnaris. Please click here to view a larger version of this figure.
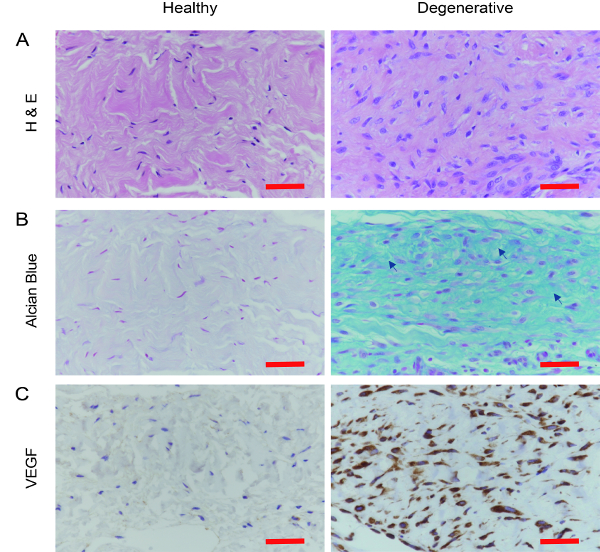
Figure 2: Confirmation of degenerative tendon histologically. (A) In the H & E staining, degenerative samples from the lateral epicondylitis had disorganized collagen bundles with loss of polarity and increased cell number compared to the healthy control. (B). Alcian blue staining showed that the degenerative tendon had increased ground substance consisting of proteoglycans and glycosaminoglycans with several mucoid patches and vacuoles between fibers (Arrow). (C). Additionally, VEGF immunohistochemistry demonstrated increased staining in vessel formation in degenerative tendon samples compared to the control samples. VEGF: Vascular endothelial growth factor. Scale bar = 50 µm. Please click here to view a larger version of this figure.
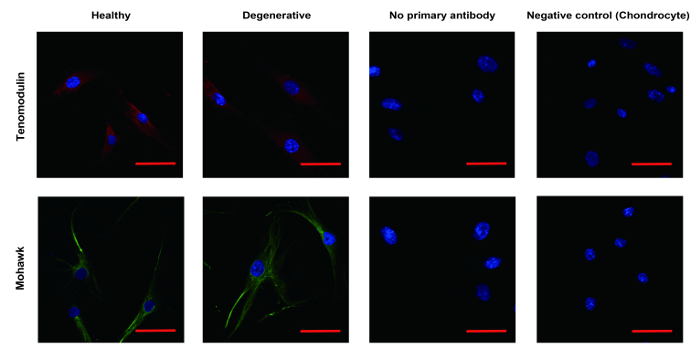
Figure 3: Identification of tenocyte by ICC. The cultured cells and cells in tendon tissue were confirmed as tenocyte by ICC. Most of the cells showed positive stain for the representative tenocyte marker, including mohawk (green) and tenomodulin (red) with elongated appearance under microscopy. Chondrocyte was used as the negative control. ICC: Immunocytochemistry. Scale bar = 50 µm. Please click here to view a larger version of this figure.
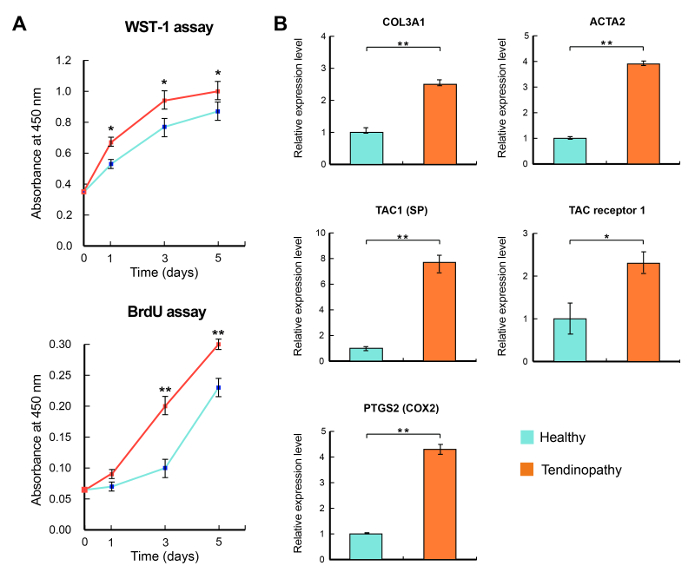
Figure 4: Characteristics of degenerative tenocyte. (A, B) Degenerative tenocytes (red) had a higher proliferation rate with a notable increase in cellularity. (C) Five genes that are known to be related in the development of tendinopathy were significantly elevated in the degenerative tenocytes. Gene expression levels were normalized against GAPDH. *: mean <0.05, **: mean <0.01, respectively. SP: substance P. Please click here to view a larger version of this figure.
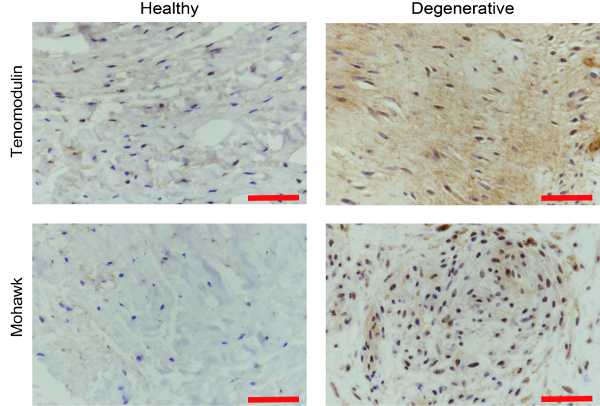
Supplementary Figure 1: Histological confirmation of the harvested tissue as the tendon tissue. The harvested tissue was also analyzed by IHC for mohawk and tenomodulin to determine whether the harvested tissue had the adequate characteristics of tendon tissue. IHC: Immunohistochemistry. Scale bar = 50 µm. Please click here to view a larger version of this figure.
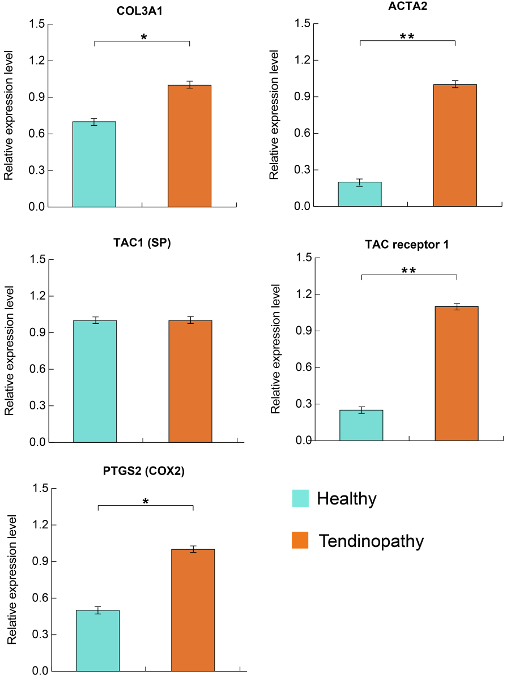
Supplementary Figure 2: Expression of tendinopathy related genes in tenocyte. The transcripts of five genes normalized by actin expression were significantly elevated in the degenerative tenocytes and have similar trends to Figure 4. Gene expression levels were normalized against actin with a mean < 0.05 and < 0.01, respectively. SP: substance P. Please click here to view a larger version of this figure.
